

The Impact of a Novel Transfer Process on Patient Bed Days and Length of Stay: A Five-Year Comparative Study at the Mayo Clinic in Rochester and Mankato Quaternary and Tertiary Care Centers
- PMID: 40566300
- PMCID: PMC12193241
- DOI: 10.3390/ijerph22060871
The Impact of a Novel Transfer Process on Patient Bed Days and Length of Stay: A Five-Year Comparative Study at the Mayo Clinic in Rochester and Mankato Quaternary and Tertiary Care Centers
Abstract
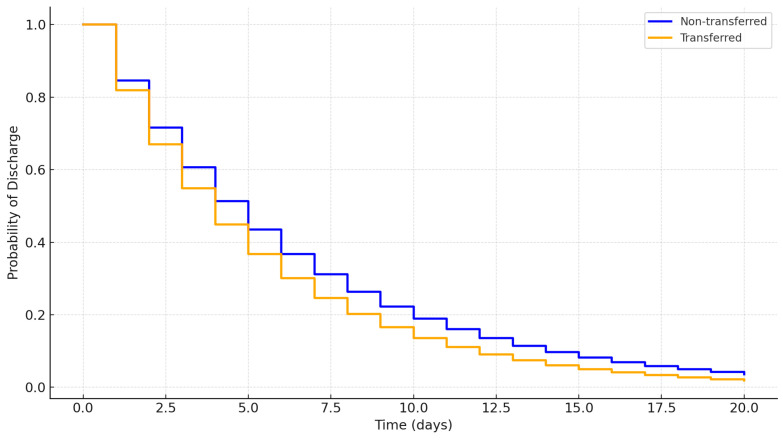
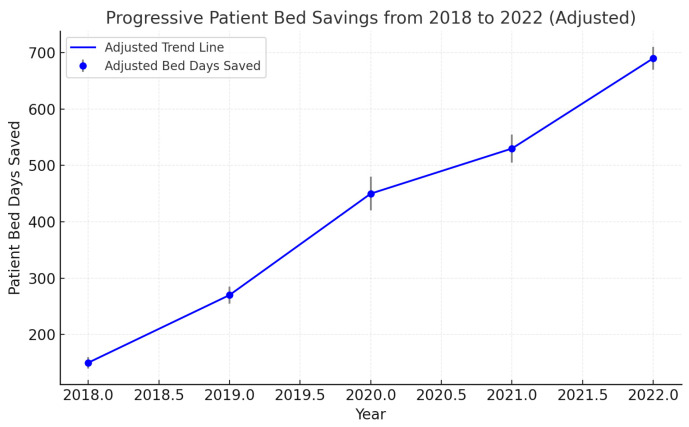
Introduction: This study evaluated the impact of parallel-level patient transfers on bed utilization efficiency within the Mayo Clinic Health System in Southern Minnesota, focusing on optimizing resources across tertiary and critical access hospitals. Methods: A retrospective analysis of 179,066 Emergency Department visits (2018-2022) was conducted, with ~2% involving parallel-level transfers for observation or admission. Machine learning was utilized to identify patients suitable for parallel transfers based on demographics, comorbidities, and clinical factors. A Random Forest model with an AUROC of 0.87 guided transfer decisions. Saved patient days were calculated as the difference between the actual LOS and the benchmark LOS based on Diagnosis-Related Groups (DRGs). Generalized estimating equations analyzed length of stay (LOS) differences, adjusted for confounders, with 95% confidence intervals (CI). Statistical analyses were conducted using SPSS (v.26). Results: The mean patient age was 56 years (SD = 17.2), with 51.4% being female. Saved patient days increased from ~600 to 5200 days over the study period. Transferred patients had a 5.7% longer unadjusted LOS compared to non-transferred patients (95% CI: 2.9-8.6%, p < 0.001). After adjustment for demographics and comorbidities, the LOS difference was not significant (adjusted mean difference: 0.4%, 95% CI: -1.7-2.5%, p = 0.51). Conclusions: Parallel-level transfers increased saved patient days, reflecting enhanced resource utilization. However, the adjusted LOS differences were not significant, highlighting the need for robust transfer protocols and controlled studies to confirm these findings.
Keywords: bed utilization efficiency; parallel transfer; saved patient days; tertiary care centers.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.Health Technol Assess. 2006 Aug;10(29):iii-iv, ix-xi, 1-133. doi: 10.3310/hta10290. Health Technol Assess. 2006. PMID: 16904048 Clinical Trial.
-
Length of stay and comorbidity prevalence among individuals with chronic obstructive pulmonary disease in a tertiary care healthcare center in Saudi Arabia; A cross-sectional study.Medicine (Baltimore). 2025 May 23;104(21):e41855. doi: 10.1097/MD.0000000000041855. Medicine (Baltimore). 2025. PMID: 40419901 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
References
-
- Appropriate Interfacility Patient Transfer American College of Emergency Physicians. [(accessed on 26 August 2023)]. Available online: https://www.acep.org/patient-care/policy-statements/appropriate-interfac....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
