

The Safety of Ultrasound-Guided Needle Approaches for Patellar Tendinopathy: A Theoretical Cadaveric Model
- PMID: 40566458
- PMCID: PMC12194407
- DOI: 10.3390/jfmk10020208
The Safety of Ultrasound-Guided Needle Approaches for Patellar Tendinopathy: A Theoretical Cadaveric Model
Abstract
Background: Patellar tendinopathy is a musculoskeletal pain condition capable of impairing physical or sport activities. Preliminary evidence supports the efficacy of percutaneous electrolysis (PE) in reducing pain and related disability in patients with patellar tendinopathy.
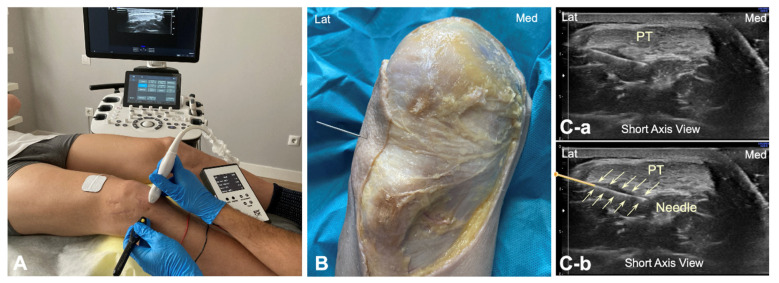
Objective: This study proposes a theoretical model for the application of a percutaneous electrolysis approach targeting the deep zone of the proximal and distal parts of the patellar tendon in both human (ultrasound-guided) and fresh cadaver (not ultrasound-guided) models.
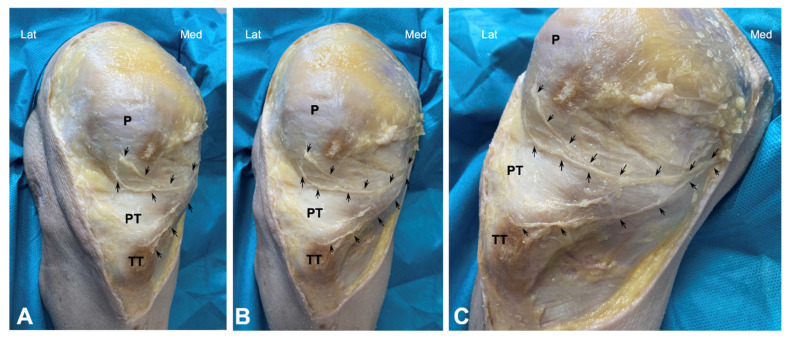
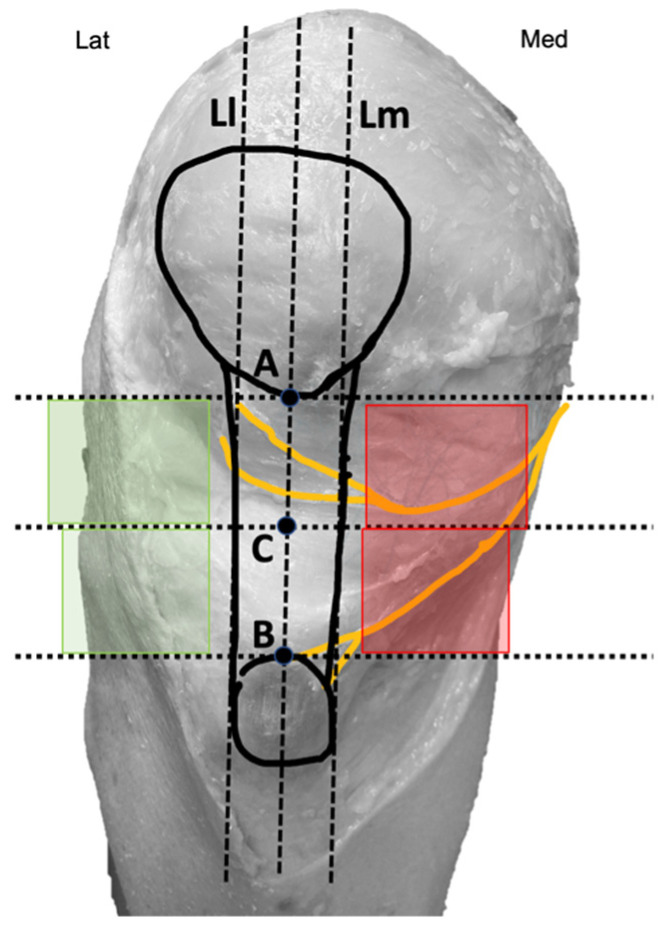
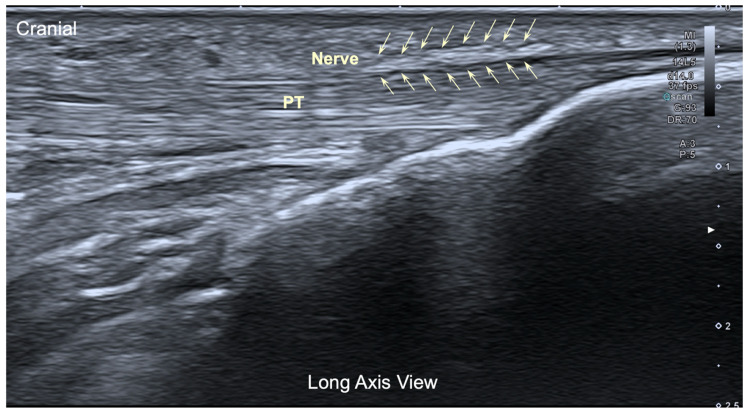
Methods: A filiform solid needle was inserted from the lateral side of the patellar tendon targeting two areas: 1, the deep proximal interface of the Hoffa's fat pad; and 2, the distal insertion of the patellar tendon at the tibial tuberosity in 10 fresh cadavers and in 10 healthy individuals. The patellar tendon, the saphenous nerve, and the infrapatellar nerve and its branches were identified by dissecting fresh cadavers to determine the anatomical trajectory of the infrapatellar nerve branches in relation to the needle.
Results: The cadaveric model shows an anatomical relationship between the patellar tendon and infrapatellar nerve branches at the medial part of the knee. Infrapatellar nerve branches ran subcutaneously obliquely from the medial to the anterior and lateral parts of the knee, crossing in front of the patellar tendon. In all cadavers, the superior and inferior infrapatellar branches ran through the superior or inferior parts of the medial knee area. Only in 2/10 knees infrapatellar nerve branches reached the lateral part of the knee, specifically the superior lateral part. No neurovascular bundle of infrapatellar nerve branches was pierced in any insertion when the needle was inserted from the lateral part of the knee.
Conclusion: This anatomical model supports the use of a lateral approach as a potentially safe approach to apply in needling interventions, e.g., percutaneous electrolysis for patellar tendinopathies. The infrapatellar nerve branches are vulnerable to needle procedures applied through the anteromedial side of the knee.
Keywords: cadaver; infrapatellar nerve; patellar tendon; percutaneous electrolysis; tendinopathy.
Conflict of interest statement
Pedro Belón-Pérez is affiliated with Real Madrid C.F. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
