

Outcomes from Quantitative Flow Ratio-Guided Complete Revascularization and Angiography-Guided Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction
- PMID: 40566730
- PMCID: PMC12178142
- DOI: 10.12659/MSM.948085
Outcomes from Quantitative Flow Ratio-Guided Complete Revascularization and Angiography-Guided Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction
Abstract
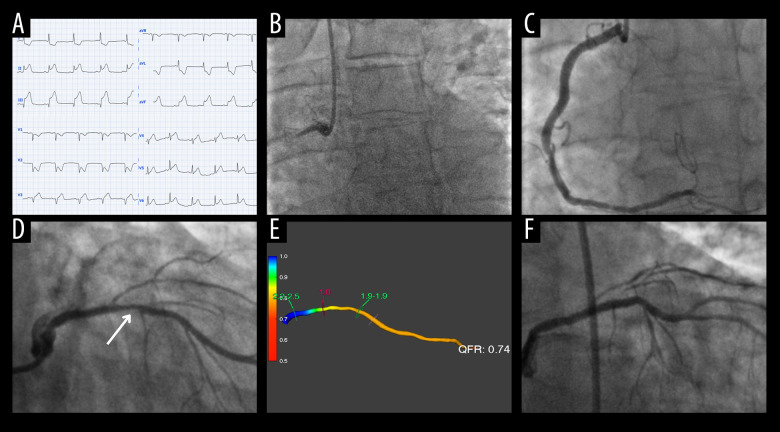
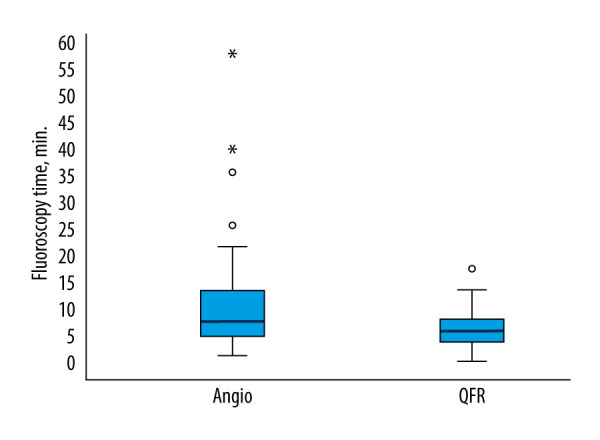
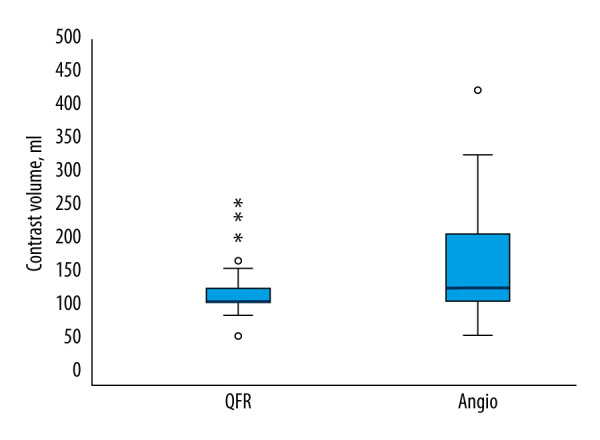
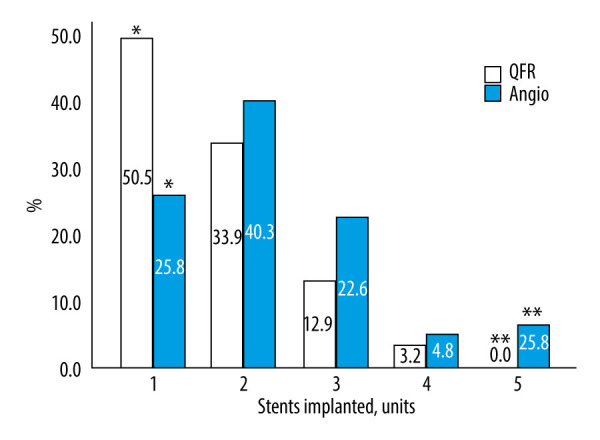
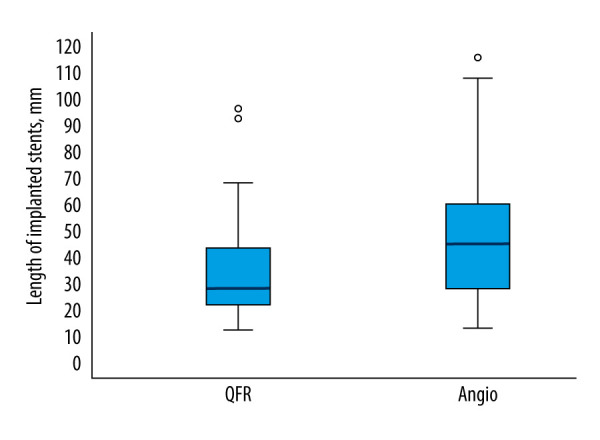
BACKGROUND Quantitative flow ratio (QFR) is a non-invasive angiographic tool that provides functional assessment of coronary stenosis without the need for pressure wires or hyperemia. This prospective study aimed to evaluate the procedural and inpatient treatment outcomes of QFR-guided percutaneous coronary intervention (PCI) compared with that of angiography-guided PCI in patients with ST-elevation myocardial infarction (STEMI) undergoing staged revascularization of non-culprit lesions. MATERIAL AND METHODS This randomized prospective single-center study was conducted at the Hospital of the Lithuanian University of Health Sciences Kaunas Clinics (July 2020-June 2021). After successful culprit-lesion PCI for STEMI, 124 participants with residual angiographically significant non-culprit stenosis (50-75%) were randomized to QFR-guided (n=62) or angiography-guided PCI (n=62). Procedural characteristics, fluoroscopy time, contrast usage, stent number/length, and inpatient treatment outcomes were compared between groups using SPSS 28.0 software. RESULTS Compared with PCI guided by visual estimation alone, the QFR-guided PCI group showed significant reductions in fluoroscopy time (median 6.2 vs 8.0 min, P=0.009), contrast volume (median 100 vs 120 mL, P=0.038), number of stents implanted (median 1.5 vs 2.0, P=0.002), and stent length (median 28 vs 45 mm, P<0.001). No significant differences were found between the groups in terms of periprocedural complications or length of inpatient stay. CONCLUSIONS QFR-guided PCI of the non-culprit lesion resulted in shorter fluoroscopy time, lower contrast volume, and a smaller number and average length of implanted stents. These findings highlight the potential of QFR to enhance procedural efficiency and reduce unnecessary stenting in clinical practice without compromising patient outcomes.
Conflict of interest statement
Figures
Similar articles
-
FFR-Guided Complete or Culprit-Only PCI in Patients with Myocardial Infarction.N Engl J Med. 2024 Apr 25;390(16):1481-1492. doi: 10.1056/NEJMoa2314149. Epub 2024 Apr 8. N Engl J Med. 2024. PMID: 38587995 Clinical Trial.
-
Timing of fractional flow reserve-guided complete revascularization in patients with ST-segment elevation myocardial infarction with multivessel disease: Rationale and design of the OPTION-STEMI trial.Am Heart J. 2024 Jul;273:35-43. doi: 10.1016/j.ahj.2024.03.017. Epub 2024 Apr 18. Am Heart J. 2024. PMID: 38641031
-
Assessing angiographic results of saline autotransfusion and thrombus aspiration in STEMI patients.Future Cardiol. 2025 Mar;21(4):237-243. doi: 10.1080/14796678.2025.2472581. Epub 2025 Mar 4. Future Cardiol. 2025. PMID: 40035694
-
Optimal Strategy for Complete Revascularization in ST-Segment Elevation Myocardial Infarction and Multivessel Disease: A Network Meta-Analysis.J Am Coll Cardiol. 2025 Jan 7;85(1):19-38. doi: 10.1016/j.jacc.2024.09.1231. J Am Coll Cardiol. 2025. PMID: 39779054
-
Complete versus culprit-only revascularisation in ST elevation myocardial infarction with multi-vessel disease.Cochrane Database Syst Rev. 2017 May 3;5(5):CD011986. doi: 10.1002/14651858.CD011986.pub2. Cochrane Database Syst Rev. 2017. PMID: 28470696 Free PMC article.
References
-
- Barauskas M, Žiubrytė G, Barauskienė G, et al. Systemic analysis of diagnostic performance and agreement between fractional flow reserve and quantitative flow ratio. Cor Vasa. 2021;63(6):683–87.
-
- Andersen BK, Sejr-Hansen M, Maillard L, et al. Quantitative flow ratio versus fractional flow reserve for coronary revascularisation guidance (FAVOR III Europe): A multicentre, randomised, non-inferiority trial. Lancet. 2024;404(10465):1835–46. [published correction appears in Lancet. 2025;404(10471):2542] - PubMed
-
- Barauskas M, Žiubrytė G, Jodka N, Unikas R. Quantitative flow ratio for assessment of non-culprit coronary artery lesions during percutaneous coronary intervention (PCI) in 79 patients diagnosed with ST-elevation myocardial infarction (STEMI): A study from a single center in Lithuania. Med Sci Monit. 2023;29:e939360. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
