

Acromioclavicular Fixation Before Coracoclavicular Tunnel Placement and Acromioclavicular Construct Design Improved Reduction and Stability in a Whole-Shoulder Girdle Model: A Pilot Study
- PMID: 40566939
- PMCID: PMC12235056
- DOI: 10.1177/03635465251349143
Acromioclavicular Fixation Before Coracoclavicular Tunnel Placement and Acromioclavicular Construct Design Improved Reduction and Stability in a Whole-Shoulder Girdle Model: A Pilot Study
Abstract
Background: Reconstruction of the acromioclavicular (AC) ligament after an acute AC dislocation as the first surgical step before coracoclavicular (CC) tunnel placement has been proposed to reduce the risk of postoperative loss of reduction. Additional reconstruction of AC ligamentous complex lesions with different types of bracing constructs has also been described to improve outcomes. Still, the effect of the sequence of surgical steps and the AC bracing construct design on the AC kinematics in a whole-shoulder girdle model has not been reported.
Hypothesis: The primary hypothesis was that postoperative AC joint reduction would improve when the AC joint was reconstructed before CC tunnel placement. The secondary hypothesis was that different AC bracing construct designs affect joint kinematics during physiological motion in a whole-shoulder girdle model.
Study design: Controlled laboratory study.
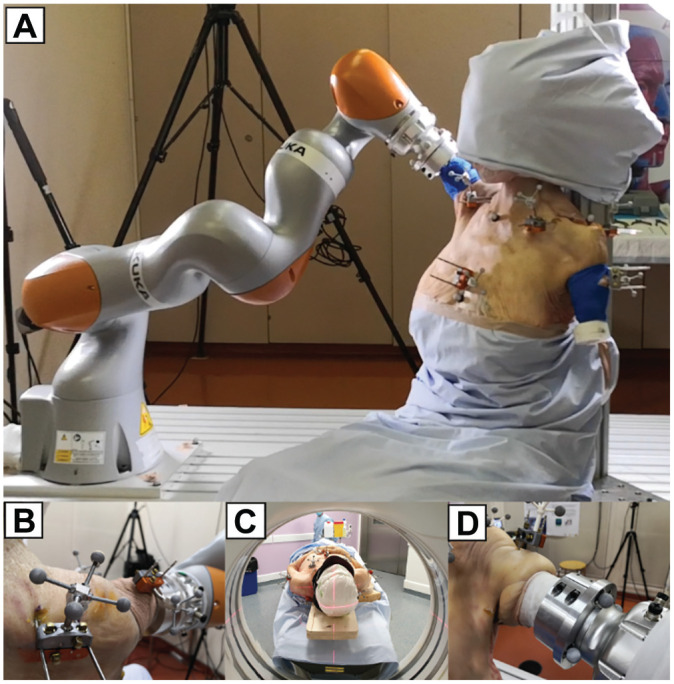
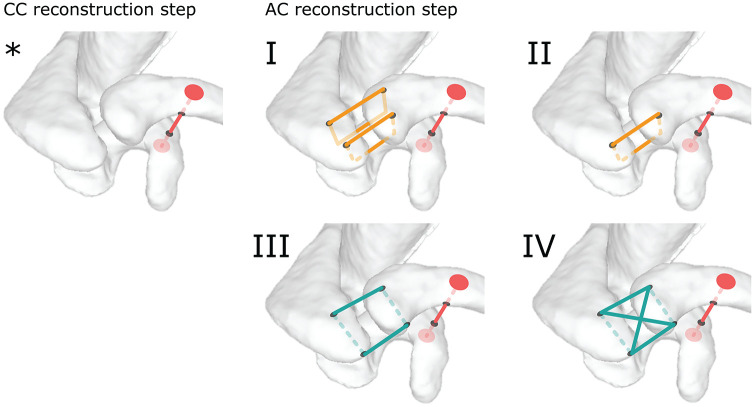
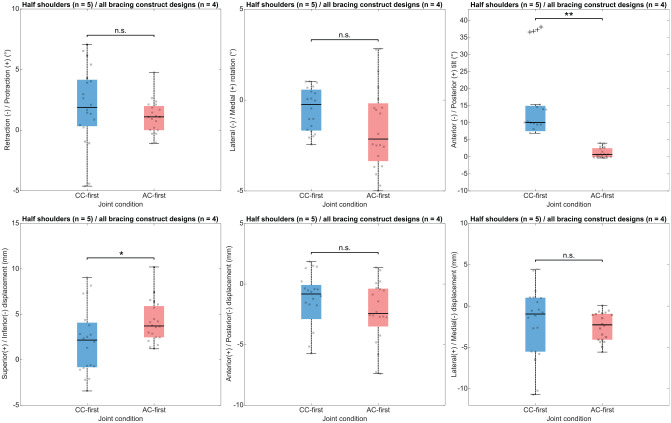
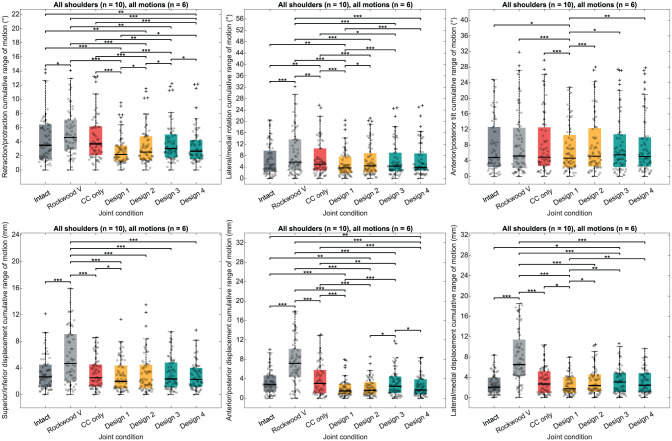
Methods: Five cadaveric specimens (10 shoulders) were prepared for whole-shoulder mobilization with a robotic manipulator. Joint kinematics was acquired during physiological motions using an optical motion capture system. Recorded parameters were (1) the joint reduction in a resting position, expressed as joint displacements and rotations compared with an intact AC joint, and (2) the joint stability during all tested motions, expressed as joint displacements and rotations. The tested joint conditions were intact AC joint, induced Rockwood type 5 lesion, isolated CC reconstruction, and 4 AC joint bracing construct designs. AC reconstruction was performed before (AC-first technique) and after (CC-first technique) CC tunnel placement in 5 shoulders each.
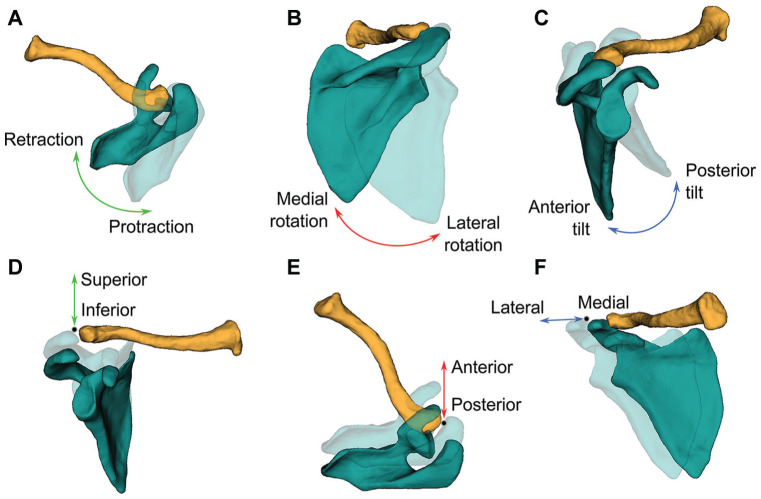
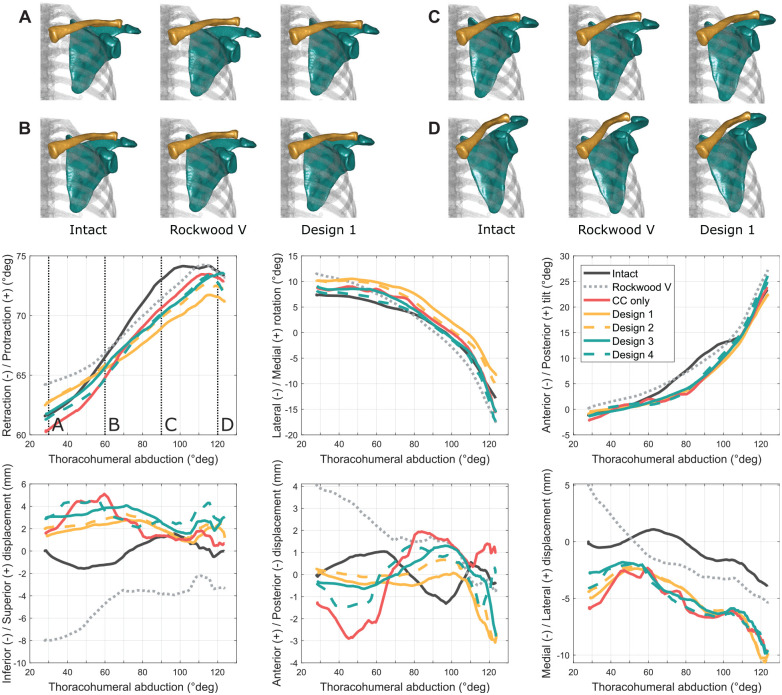
Results: The AC-first surgical step improved the AC joint reduction in anterior-posterior tilt compared with CC-first (median difference, -9.4°; P < .001). The AC-first surgical step also demonstrated an increased superior-inferior joint reduction with hyperreduction (median difference, 1.6 mm; P = .041) compared with CC-first. Dispersion of joint reduction values was reduced with the AC-first step and particularly for anterior-posterior tilt (IQR difference, -4.8°) and lateral-medial displacement (IQR difference, -3.4 mm). The double vertical bracing construct design increased the AC joint stability compared with other constructs and reached a statistical significance in all rotational displacement (P < .001 to P = .041) as well as in lateral-medial displacement (P = .001 to P = .015).
Conclusion: The AC-first surgical step sequence improved AC joint alignment in the scapular sagittal plane and increased joint hyperreduction. The double vertical bracing construct design achieved the highest joint stability over other tested designs during passive motion.
Clinical relevance: The restoration of the preinjury joint alignment and the optimization of the joint stability may improve outcomes and reduce the risk of construct de-tensioning during the rehabilitation phase.
Keywords: acromioclavicular lesion; bracing construct design; cadaveric specimen; joint kinematics; robotic manipulator; surgical step sequence; whole shoulder.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Department of Surgery of the Geneva University Hospitals. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Kinematic analysis of the sternoclavicular, acromioclavicular and scapulothoracic joint demonstrates significant multiplanar alterations in acromioclavicular injuries with each consecutive ligamentous injury during movements of the shoulder girdle: A whole-cadaver study.Knee Surg Sports Traumatol Arthrosc. 2025 Jul;33(7):2614-2625. doi: 10.1002/ksa.12621. Epub 2025 Feb 20. Knee Surg Sports Traumatol Arthrosc. 2025. PMID: 39976155
-
Effect of deltoid-trapezius overlap repair on acromioclavicular joint stability: a biomechanical study using fresh-frozen cadavers.BMC Musculoskelet Disord. 2025 Jul 4;26(1):611. doi: 10.1186/s12891-025-08883-7. BMC Musculoskelet Disord. 2025. PMID: 40616040 Free PMC article.
-
Suture stabilization of the acromioclavicular ligament plus clavicular hook plate fixation vs. total ligament repair with loop plates for acromioclavicular joint dislocation.J Orthop Surg Res. 2025 Aug 8;20(1):746. doi: 10.1186/s13018-025-06032-3. J Orthop Surg Res. 2025. PMID: 40781636 Free PMC article.
-
Coracoclavicular ligament reconstruction: a systematic review and a biomechanical study of a triple endobutton technique.Medicine (Baltimore). 2014 Dec;93(28):e193. doi: 10.1097/MD.0000000000000193. Medicine (Baltimore). 2014. PMID: 25526435 Free PMC article.
-
Acromioclavicular reconstruction techniques after acromioclavicular joint injuries: A systematic review of biomechanical studies.Clin Biomech (Bristol). 2023 Jan;101:105847. doi: 10.1016/j.clinbiomech.2022.105847. Epub 2022 Dec 5. Clin Biomech (Bristol). 2023. PMID: 36521410
References
-
- Abrams GD, McGarry MH, Jain NS, et al. Biomechanical evaluation of a coracoclavicular and acromioclacicular ligament reconstruction technique utilizing a single continuous intramedullary free tendon graft. J Shoulder Elbow Surg. 2013;22(7):979-985. - PubMed
-
- Barth J, Duparc F, Andrieu K, et al. Is coracoclavicular stabilisation alone sufficient for the endoscopic treatment of severe acromioclavicular joint dislocation (Rockwood types III, IV, and V)? Orthop Traumatol Surg Res. 2015;101(8 suppl):S297-S303. - PubMed
-
- Beitzel K, Obopilwe E, Apostolakos J, et al. Rotational and translational stability of different methods for direct acromioclavicular ligament repair in anatomic acromioclavicular joint reconstruction. Am J Sports Med. 2014;42(9):2141-2148. - PubMed
-
- Boileau P, Alami G, Rumian A, et al. The doubled-suture Nice knot. Orthopedics. 2017;40(2):e382-e386. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
