

Genomic Epidemiology of Respiratory Syncytial Virus in a New England Hospital System, 2024
- PMID: 40567998
- PMCID: PMC12188213
- DOI: 10.1093/ofid/ofaf334
Genomic Epidemiology of Respiratory Syncytial Virus in a New England Hospital System, 2024
Abstract
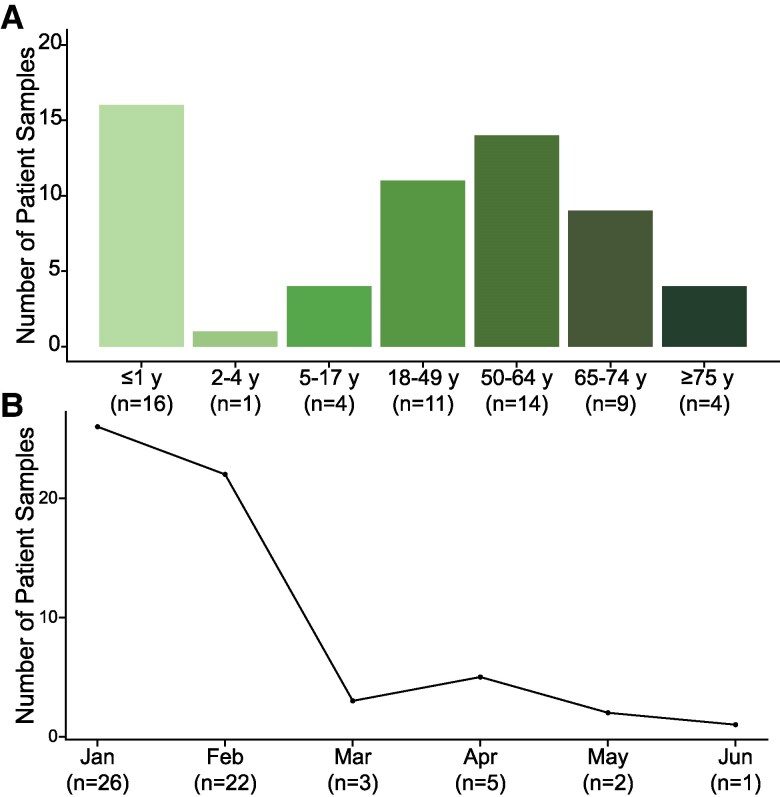
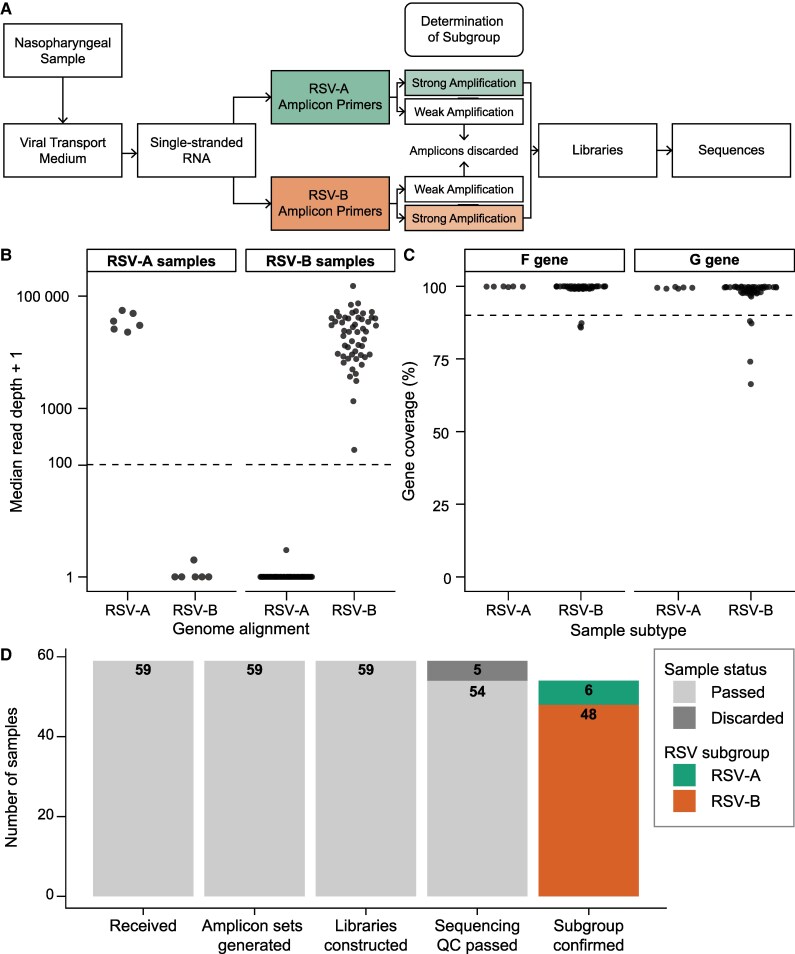
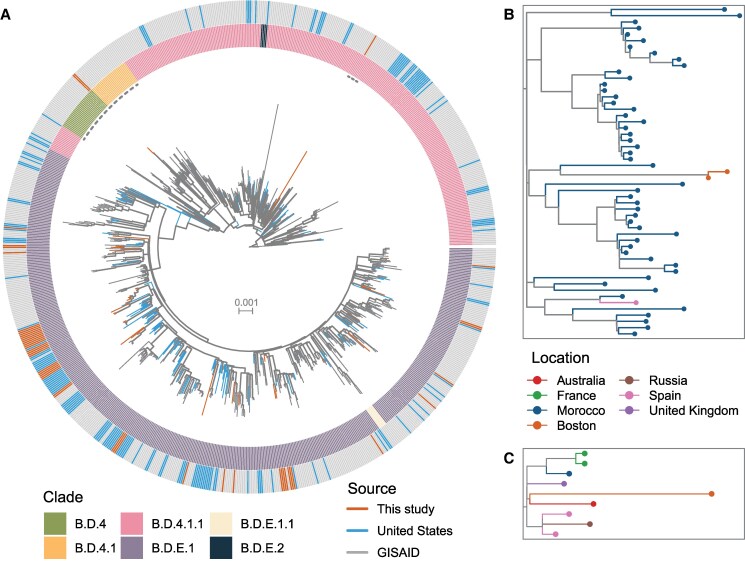
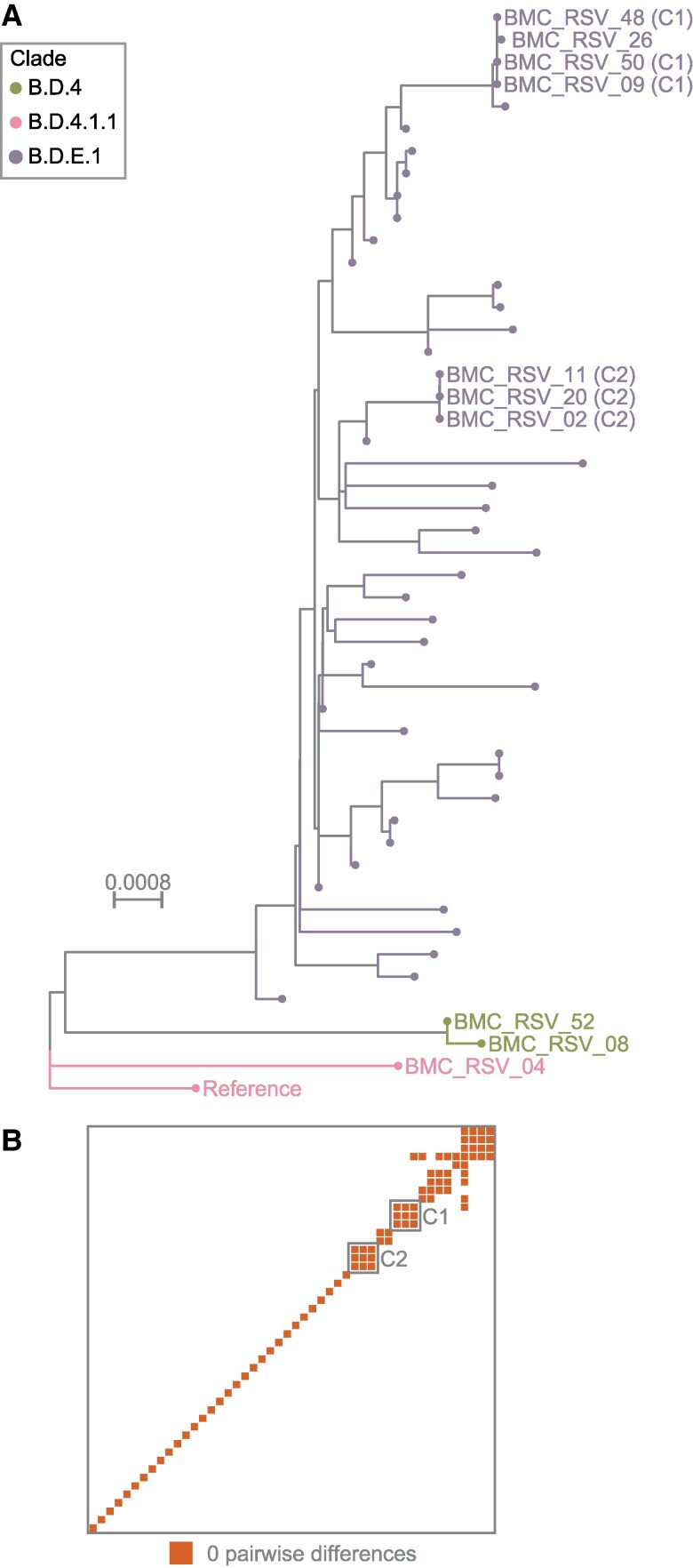
Respiratory syncytial virus (RSV) is one of the main seasonal respiratory pathogens in the United States. Although several RSV vaccines were recently approved, vaccination rates remain low. We analyzed RSV-positive nasopharyngeal swabs from Boston Medical Center in 2024 using amplicon-based whole genome sequencing. We found that >80% of the samples were RSV-B, representing a major switch from 2022, when Boston RSV samples were approximately 90% RSV-A. Forty-five of 48 RSV-B samples mapped into a single clade (B.D.E.1), though not a single source within it, suggesting that the predominance of RSV-B is multifactorial. We also found examples of highly related genomes, suggesting clustered transmission. Mutations associated with vaccine escape were not observed. Our work highlights the importance of genomic surveillance for respiratory pathogens to monitor transmission dynamics, such as the unexpected switch from RSV-A to RSV-B dominance, and to understand the epidemiological changes that may be associated with RSV interventions.
Keywords: Massachusetts; genomic epidemiology; genomic surveillance; respiratory infections; respiratory syncytial virus.
© The Author(s) 2025. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest.
Figures
References
-
- Saravanos GL, Ramos I, Britton PN, Wood NJ. Respiratory syncytial virus subtype circulation and associated disease severity at an Australian paediatric referral hospital, 2014–2018. J Paediatr Child Health 2021; 57:1190–5. - PubMed
LinkOut - more resources
Full Text Sources
