

A meta-analysis of randomized controlled trials examining the effectiveness of carbetocin in reducing intraoperative blood loss during abdominal myomectomy
- PMID: 40568196
- PMCID: PMC12187817
- DOI: 10.3389/fmed.2025.1590144
A meta-analysis of randomized controlled trials examining the effectiveness of carbetocin in reducing intraoperative blood loss during abdominal myomectomy
Abstract
Aim: This study aimed to systematically review and meta-analyze randomized controlled trials (RCTs) assessing the clinical efficacy and safety of carbetocin compared to passive control (placebo or no treatment) in the context of abdominal myomectomy.
Methods: Six sources of information underwent screening until 13 April 2024. The risk of bias was assessed using the Cochrane Collaboration tool. The results were presented as mean difference (MD) or risk ratio (RR) along with a 95% confidence interval (CI) using a random-effects model.
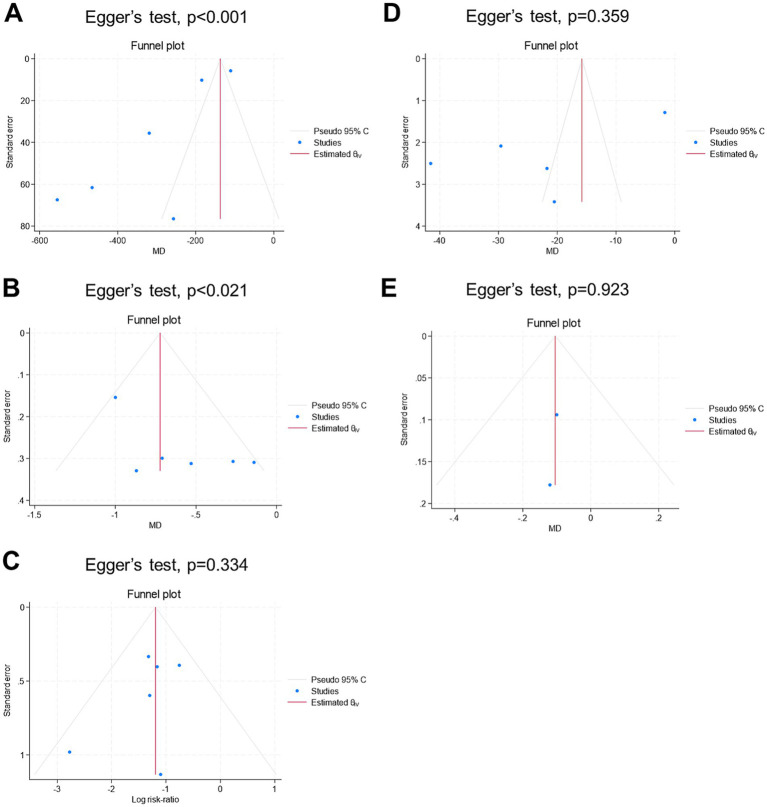
Results: Five RCTs with 6 arms and 484 patients (carbetocin = 262 and control = 222) were analyzed. The overall risk of bias was "low" in two studies and "some concerns" in three studies. The carbetocin group exhibited significantly lower mean intraoperative blood loss (n = 6 arms, MD = -292.27 mL, 95% CI [-372.5, -212.03], p < 0.001, with very low certainty of evidence), mean change in hemoglobin (n = 6 arms, MD = -0.63 g/dL, 95% CI [-0.94, -0.33], p < 0.001, with low certainty of evidence), rate of blood transfusion (RR = 0.3, 95% CI [0.21, 0.44], p < 0.001, with very low certainty of evidence), and mean operation time (n = 5 arms, MD = -22.98 min, 95% CI [-38.93, -7.02], p < 0.001, with low certainty of evidence). There was no significant difference between both groups regarding the mean hospital stay (n = 2 arms, MD = -0.1 days, 95% CI [-0.27, 0.06], p = 0.21). The sensitivity analyses demonstrated robustness across all outcomes. No major toxicities were reported.
Conclusion: Carbetocin use was tolerable and associated with considerable declines in intraoperative blood loss and related complications compared with passive control intervention during abdominal myomectomy.
Keywords: bleeding; carbetocin; leiomyoma; meta-analysis; myomectomy.
Copyright © 2025 Abu-Zaid, Baradwan, Hafedh, Alshahrani, Al Baalharith, Badghish, Algreisi, Jamjoom, Alqarni, Albelwi, Nazer, Baradwan, Alsehaimi, Alsabban and Alomar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Hypnosis for pain management during labour and childbirth.Cochrane Database Syst Rev. 2016 May 19;2016(5):CD009356. doi: 10.1002/14651858.CD009356.pub3. Cochrane Database Syst Rev. 2016. PMID: 27192949 Free PMC article.
-
Acupuncture for treating overactive bladder in adults.Cochrane Database Syst Rev. 2022 Sep 23;9(9):CD013519. doi: 10.1002/14651858.CD013519.pub2. Cochrane Database Syst Rev. 2022. PMID: 36148895 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Mettler L, Schollmeyer T, Tinelli A, Malvasi A, Alkatout I. Complications of uterine fibroids and their management, surgical Management of Fibroids, laparoscopy and hysteroscopy versus hysterectomy, Haemorrhage, adhesions, and complications. Obstet Gynecol Int. (2012) 2012:791248: 1–8. doi: 10.1155/2012/791248, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous