

Global, regional, and national burden of orofacial clefts, 1990-2021: an analysis of data from the global burden of disease study 2021
- PMID: 40568198
- PMCID: PMC12187660
- DOI: 10.3389/fmed.2025.1609700
Global, regional, and national burden of orofacial clefts, 1990-2021: an analysis of data from the global burden of disease study 2021
Abstract
Background: Orofacial clefts (OFCs) are congenital craniofacial malformation caused by embryonic developmental abnormalities, characterized by incomplete fusion of the upper lip and/or palate, leading to feeding difficulties, speech impairments, and other functional challenges. OFCs represent the most prevalent congenital malformations of oral and maxillofacial region. We aim to characterize disease burden of OFCs across regions and countries, analyze temporal trends from 1990 to 2021, examine relationship with Socio-demographic Index (SDI), explore gender disparities and predict future epidemiological patterns.
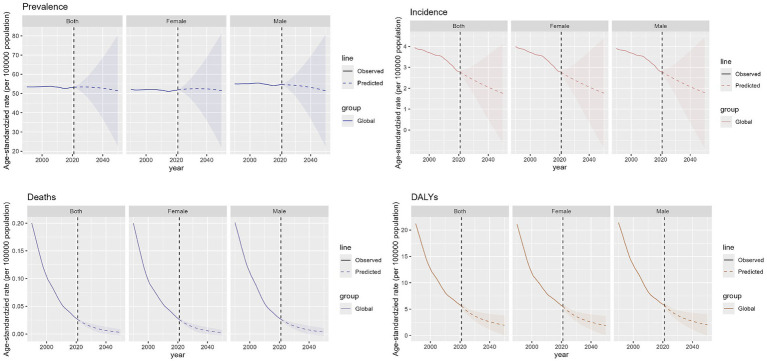
Methods: Utilizing GBD 2021 database for 204 countries/regions, we analyzed age-standardized metrics including disability-adjusted life years (DALYs), prevalence, mortality, incidence, using tools like DisMod-MR 2.1 for Bayesian meta-regression. SDI, calculated from educational attainment, per capita income, and fertility rates (range 0-1), stratified nations into quintiles. Statistical analyses included SDI-burden correlations and future projections using Bayesian age-period-cohort (BAPC) modeling, implemented through R software.
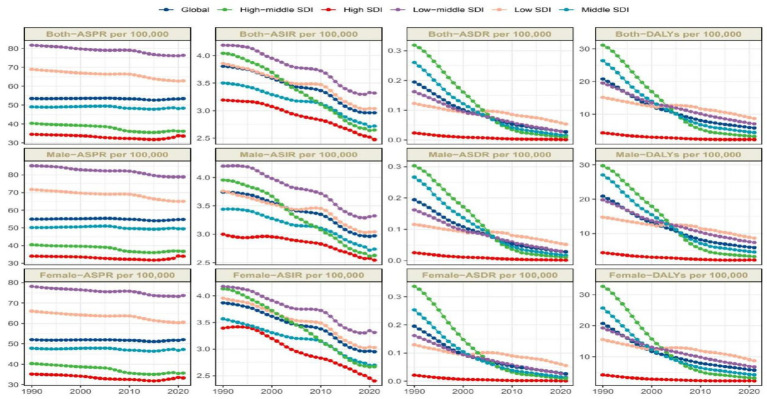
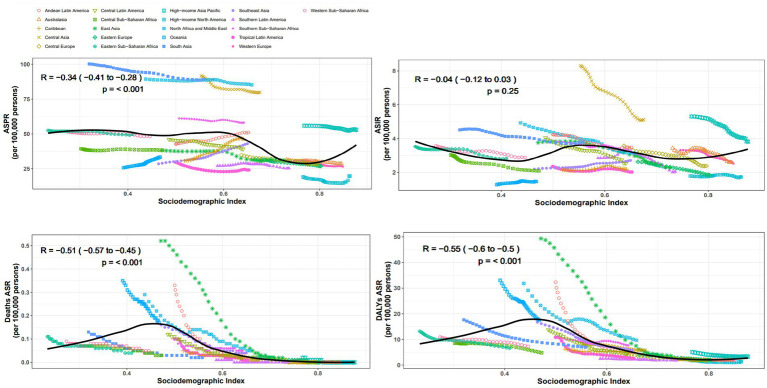
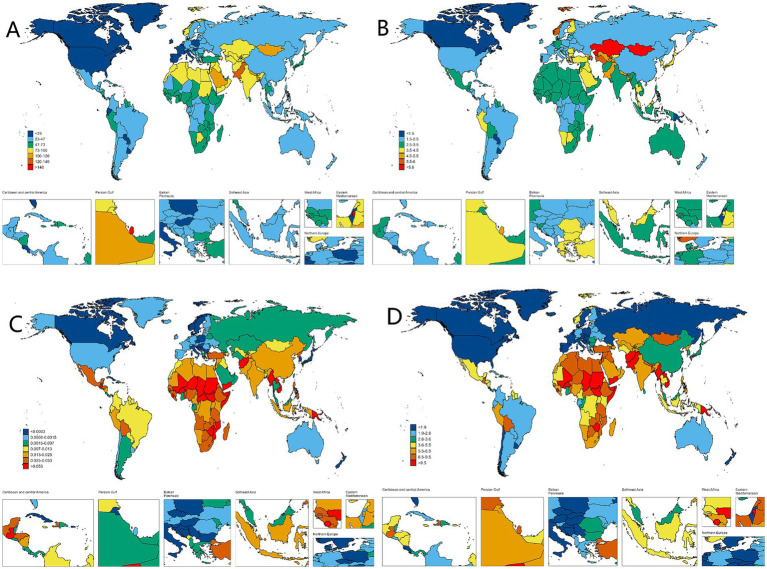
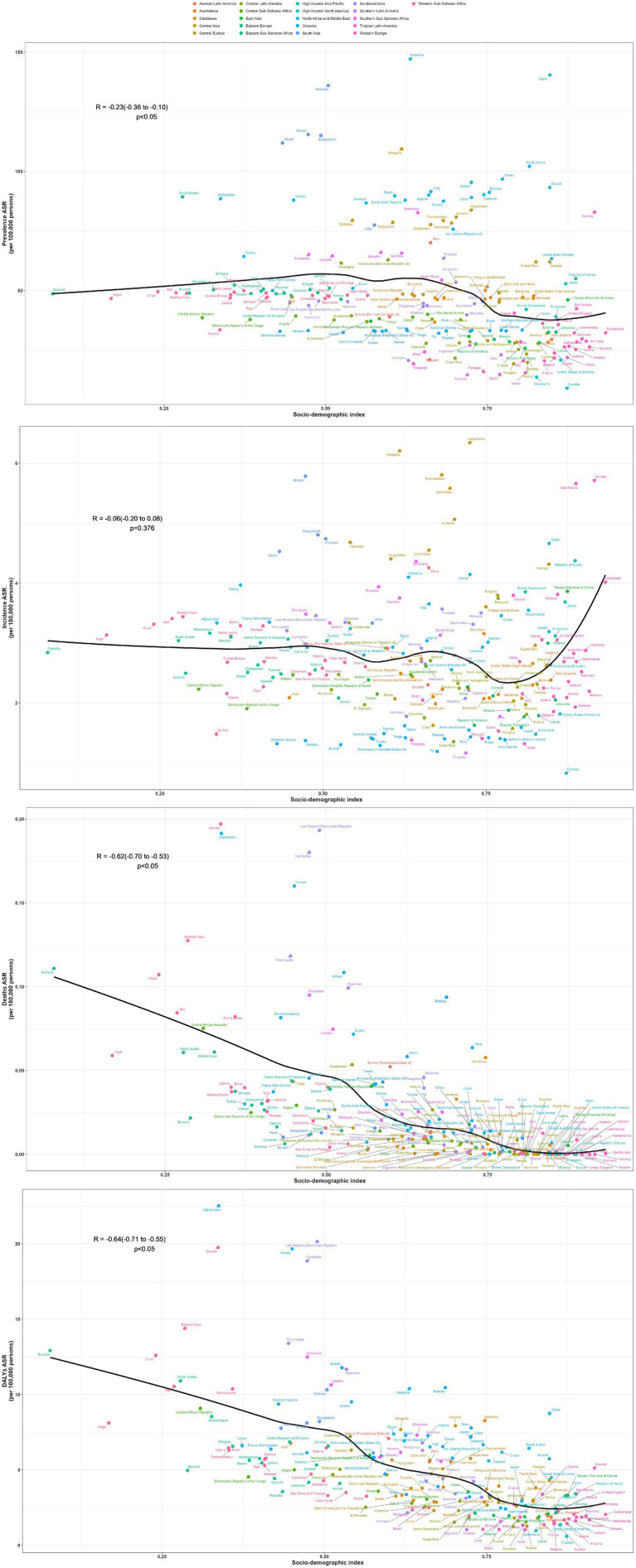
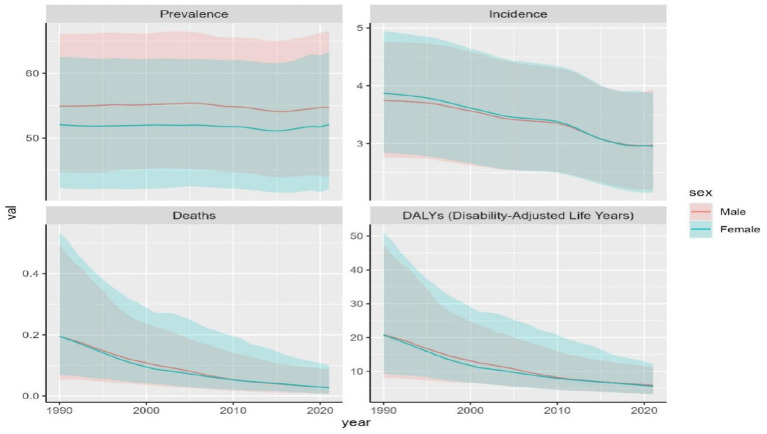
Results: In 2021, there are a total of 4124006.8 cases of OFCs worldwide, with an age-standardized prevalence rate (ASPR) of 53.4 per 100,000 (95% UI: 43-64). The age-standardized incidence rate (ASIR) was 3.0 per 100,000 (95% UI: 2.2-3.9), while age-standardized deaths rate (ASDR) of 0 per 100,000 (95% UI: 0-0.1). Additionally, age-standardized DALYs rate was 5.8 per 100,000 (95% UI: 3.5-9.8). Regionally, low- to middle-SDI regions demonstrated the highest ASPR and ASIR, whereas low-SDI areas showed the most severe ASDR and DALYs rate. In contrast, high-SDI regions consistently exhibited the lowest burden across all metrics. At the subregional level, South Asia recorded the greatest ASPR, while Central Asia had the peak ASIR. Oceania displayed the highest ASDR and DALYs rate. Country-specific analysis identified Palestine with the maximum ASPR, Kazakhstan with the highest ASIR, Papua New Guinea with the greatest ASDR, and Afghanistan with the most elevated DALYs rate.
Conclusion: The global OFCs burden demonstrated consistent decline from 1990-2021, with persistent male predominance. Regional disparities correlate strongly with SDI, particularly affecting Central Asia, South Asia, and Africa populations.
Keywords: DALY (disability-adjusted life years); GBD (2021) database; cleft lip and palate; disease burden analysis; incidence; prevalence.
Copyright © 2025 Wang, Qi, Chen and Niu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
The global, regional, and national brain and central nervous system cancer burden and trends from 1990 to 2021: an analysis based on the Global Burden of Disease Study 2021.Front Neurol. 2025 Jun 18;16:1574614. doi: 10.3389/fneur.2025.1574614. eCollection 2025. Front Neurol. 2025. PMID: 40606128 Free PMC article.
-
Global, regional, and national burden of maternal disorders, 1990-2021: a systematic analysis from the global burden of disease study 2021.BMC Public Health. 2025 Jul 29;25(1):2576. doi: 10.1186/s12889-025-23814-w. BMC Public Health. 2025. PMID: 40730990 Free PMC article.
-
Global, regional, and national burden of endometriosis among women of childbearing age from 1990 to 2021: a cross-sectional analysis from the 2021 global burden of disease study.Int J Surg. 2025 Jun 20. doi: 10.1097/JS9.0000000000002647. Online ahead of print. Int J Surg. 2025. PMID: 40540534
-
National and subnational burden of brain and central nervous system cancers in China and global from 1990 to 2021: results from the global burden of disease study 2021.Arch Public Health. 2025 Jul 28;83(1):195. doi: 10.1186/s13690-025-01683-4. Arch Public Health. 2025. PMID: 40722045 Free PMC article.
-
Global, regional, and national burden of shoulder dislocation 1990-2021: a systematic analysis of the Global Burden of Disease study 2021.J Shoulder Elbow Surg. 2025 May 9:S1058-2746(25)00379-9. doi: 10.1016/j.jse.2025.03.037. Online ahead of print. J Shoulder Elbow Surg. 2025. PMID: 40349910 Review.
References
LinkOut - more resources
Full Text Sources