

Donation after circulatory death with thoracoabdominal normothermic regional perfusion recovery has similar outcomes with donation after brain death for lung transplantation
- PMID: 40568346
- PMCID: PMC12192336
- DOI: 10.1016/j.jhlto.2025.100289
Donation after circulatory death with thoracoabdominal normothermic regional perfusion recovery has similar outcomes with donation after brain death for lung transplantation
Abstract
Introduction: Donation after circulatory death (DCD) with thoracoabdominal normothermic regional perfusion (TA-NRP) has been increasingly used to procure cardiac allografts; however, concerns persist regarding its impact on lung allografts. We present our institution's experience with DCD TA-NRP and donation after brain death (DBD) lung transplants, comparing outcomes between the two techniques.
Methods: All lung transplants recovered with DBD or DCD TA-NRP performed between October 2022 and December 2024 were included. DCD TA-NRP procured lungs were retrieved using a lung protective strategy including early reintubation and pulmonary venting as previously described. The primary outcome was survival, with secondary outcomes of primary graft dysfunction (PGD) and pulmonary-related mortality.
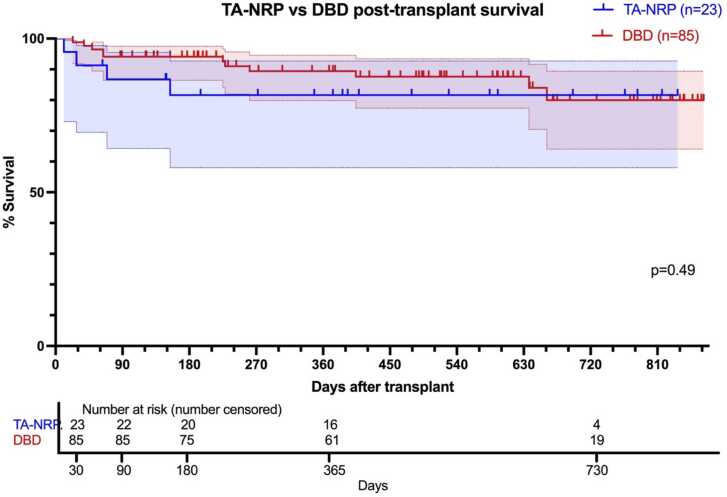
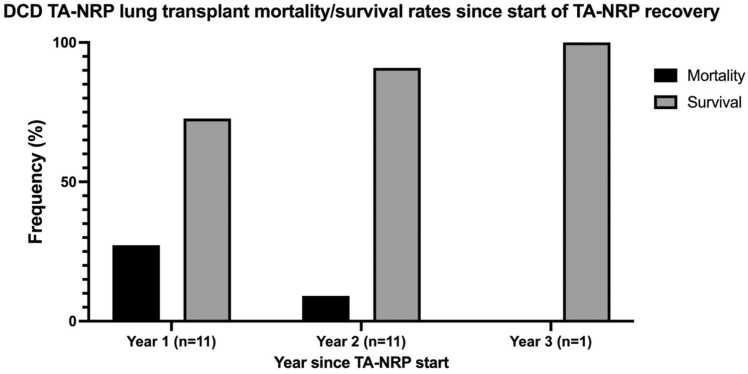
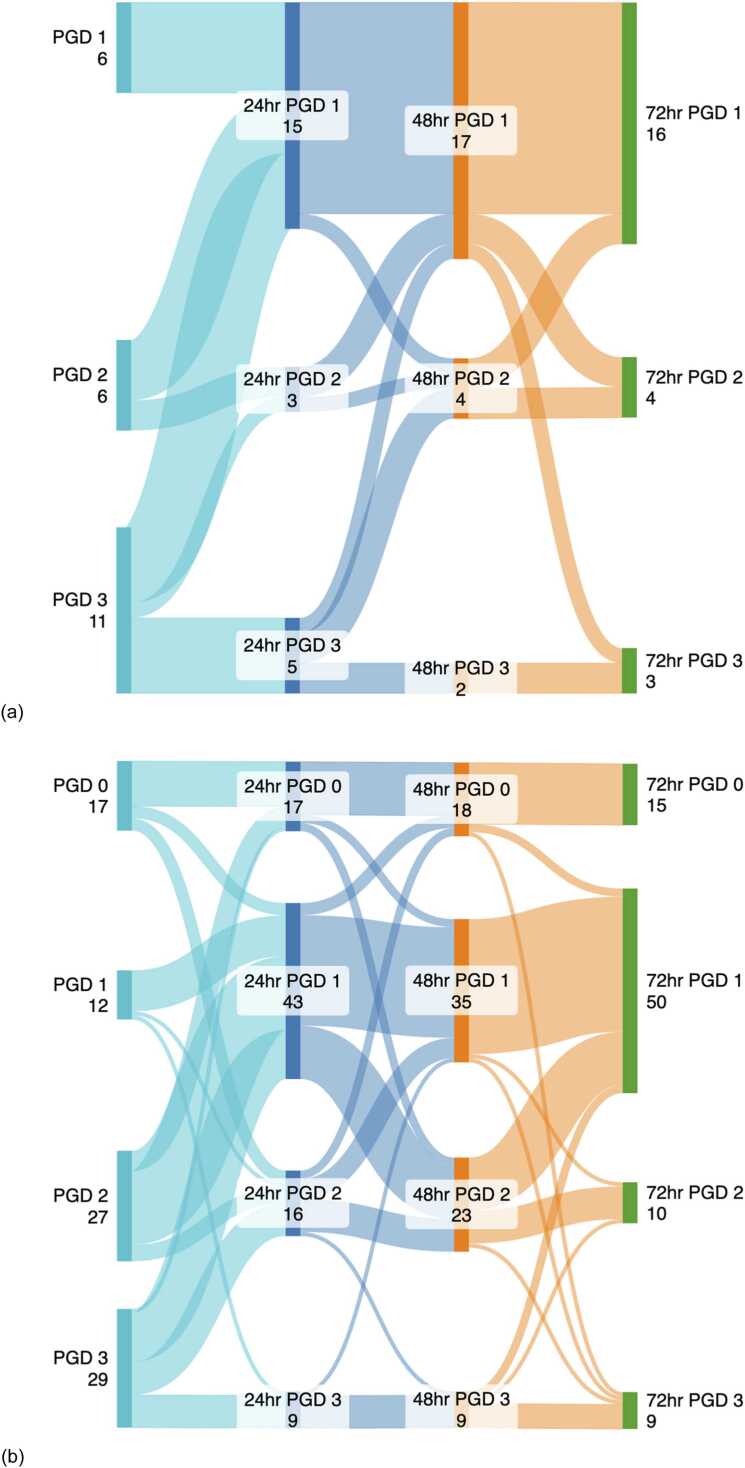
Results: There were 85 DBD and 23 DCD TA-NRP lung transplants performed in the study period. Overall survival was not significantly different by Kaplan-Meier curve (p = 0.49), with 1-year absolute survival of 81.6% for DCD TA-NRP, with only one pulmonary-related mortality, and 89.4% for DBD, with six pulmonary-related mortalities. PGD grade 3 rates were not statistically different at postoperative day (POD) 0 (47.8% DCD TA-NRP vs 35.2% DBD, p = 0.27), POD 1 (21.7% vs 10.6%, p = 0.16), POD2 (8.7% vs 11.7%, p = 0.68), and POD3 (13.0% vs 11.8%, p = 0.87). Other intraoperative and postoperative outcomes were not significantly different.
Conclusion: Lung transplantation outcomes were not significantly different between lung grafts recovered by DCD TA-NRP and DBD. This early data suggests TA-NRP may not adversely impact DCD lung allografts during procurement.
Keywords: Donation after brain death; Donation after circulatory death; Lung transplantation; Normothermic regional perfusion; Primary graft dysfunction.
© 2025 International Society for Heart and Lung Transplantation.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Direct procurement with machine perfusion and normothermic regional perfusion in donation after circulatory death heart transplantation.J Thorac Cardiovasc Surg. 2025 Jul;170(1):256-265.e6. doi: 10.1016/j.jtcvs.2024.10.033. Epub 2024 Oct 26. J Thorac Cardiovasc Surg. 2025. PMID: 39490962
-
The United Kingdom's experience of controlled donation after circulatory death direct procurement of lungs with concomitant abdominal normothermic regional perfusion with an analysis of short-term outcomes.J Heart Lung Transplant. 2025 Aug;44(8):1307-1318. doi: 10.1016/j.healun.2025.03.019. Epub 2025 Apr 1. J Heart Lung Transplant. 2025. PMID: 40180231
-
Thoracoabdominal Normothermic Regional Perfusion and Donation After Circulatory Death Lung Use.JAMA Netw Open. 2025 Feb 3;8(2):e2460033. doi: 10.1001/jamanetworkopen.2024.60033. JAMA Netw Open. 2025. PMID: 39960670 Free PMC article.
-
Lung Protection in Donation after Circulatory Death with Thoracoabdominal Normothermic Regional Perfusion.Semin Thorac Cardiovasc Surg. 2025 Jul 3:S1043-0679(25)00095-4. doi: 10.1053/j.semtcvs.2025.05.011. Online ahead of print. Semin Thorac Cardiovasc Surg. 2025. PMID: 40617513 Review.
-
Machine perfusion in liver transplantation.Cochrane Database Syst Rev. 2023 Sep 12;9(9):CD014685. doi: 10.1002/14651858.CD014685.pub2. Cochrane Database Syst Rev. 2023. PMID: 37698189 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
