

Assessment of S100A8/A9 and resistin as predictive biomarkers for mortality in critically ill patients with sepsis
- PMID: 40568710
- PMCID: PMC12188459
- DOI: 10.3389/fcimb.2025.1555307
Assessment of S100A8/A9 and resistin as predictive biomarkers for mortality in critically ill patients with sepsis
Abstract
Introduction: Sepsis is associated with high mortality. Early intervention is crucial to reducing sepsis-related mortality. This study aims to assess the clinical potential of S100A8/A9 and resistin as novel biomarkers for predicting mortality risk in sepsis patients.
Method: Serum samples were collected and analyzed from 141 adult sepsis patients (discovery cohort), 43 non-sepsis intensive care units (ICU) patients, 15 healthy volunteers, and 55 sepsis patients along with 17 non-sepsis ICU patients (validation cohort). The 28-day mortality and sequential organ failure assessment (SOFA) scores of the participants were compared. Additionally, the predictive ability of S100A8/A9 and resistin for sepsis mortality was evaluated using the area under the receiver operating characteristic curve at ICU admission.
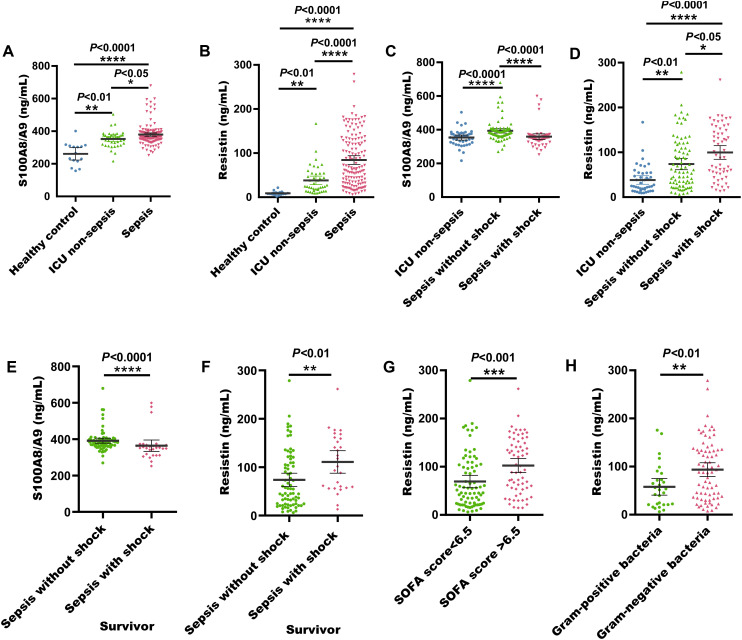
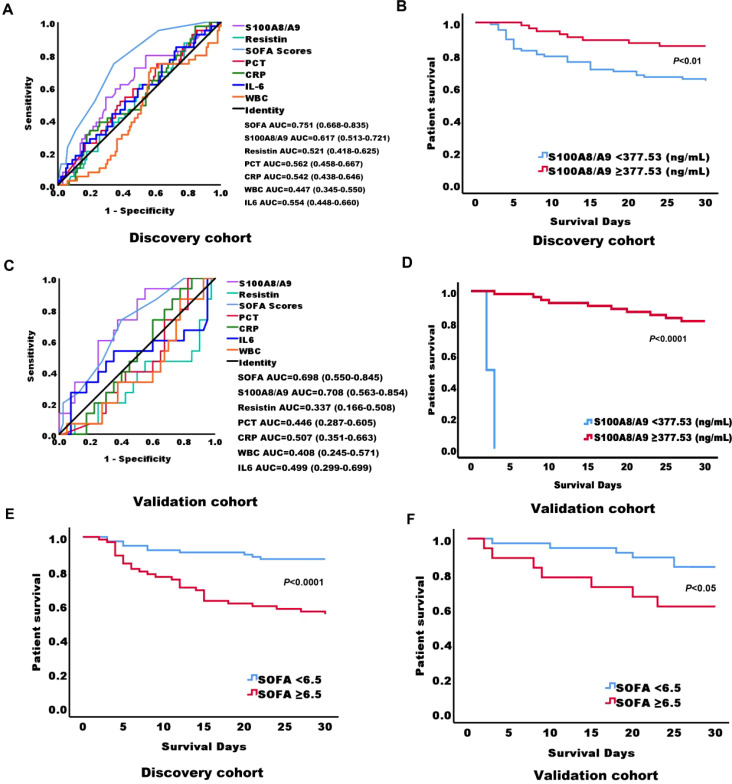
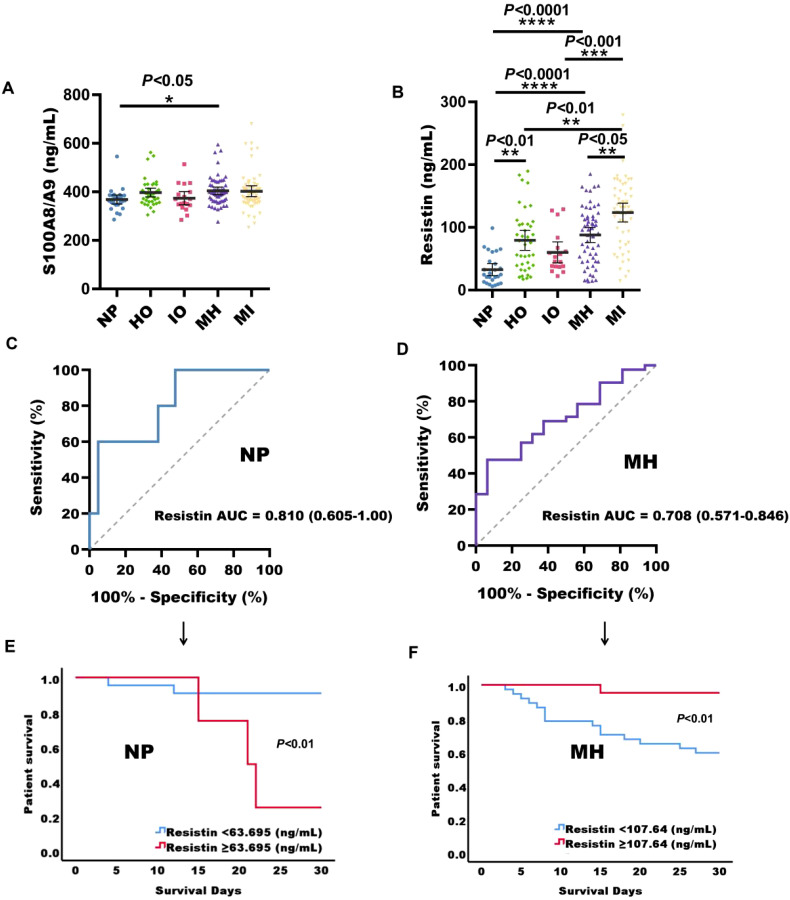
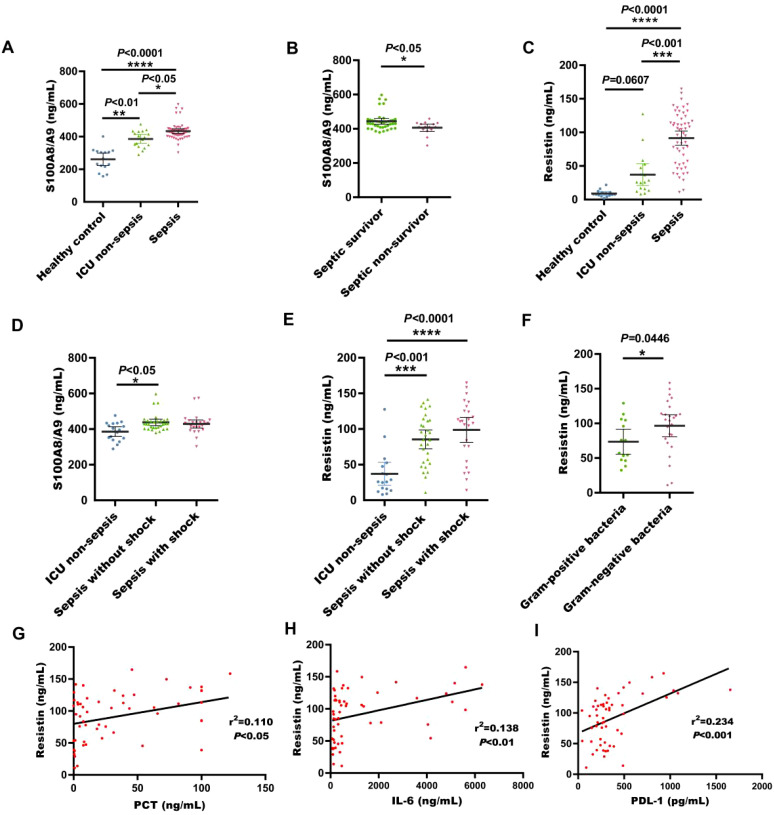
Results: The concentrations of S100A8/A9 and resistin in sepsis patients were noticeably increased relative to non-sepsis patients and healthy controls. Serum S100A8/A9 concentrations in surviving sepsis patients were significantly higher than in non-surviving patients. On the day of admission, serum resistin concentrations in Gram-negative (G-) sepsis patients were considerably elevated relative to Gram-positive (G+) infected sepsis patients. Among sepsis patients admitted to the ICU, the AUC for S100A8/A9 in predicting 28-day mortality was 0.617 (P = 0.032; 95% confidence bounds 0.513-0.721), and for SOFA was 0.750 (P < 0.0001; 95% confidence bounds 0.660-0.840). Sepsis patients with high serum S100A8/A9 concentrations (≥ 377.53 ng/mL) had a higher survival rate relative to those with low concentrations (<377.53 ng/mL). In the validation cohort, the AUC for S100A8/A9 and 28-day mortality was 0.708 (P = 0.032; 95% confidence bounds 0.563-0.854), and for SOFA was 0.698 (P = 0.025; 95% confidence bounds 0.550-0.845). Additionally, sepsis patients with high serum S100A8/A9 concentrations (≥ 377.53 ng/mL) also had a higher survival rate relative to those with lower concentrations (< 377.53 ng/mL). Furthermore, serum resistin levels in patients with a normal phenotype and mixed phenotype with hyperinflammation were predictive of mortality, with an AUC of 0.810 (P = 0.034; 95% confidence bounds 0.605-1.00) and 0.708 (P = 0.015; 95% confidence bounds 0.571-0.846). In patients with a normal sepsis phenotype, those with high serum resistin levels (≥ 63.695 ng/mL) had a lower survival rate compared to those with low resistin levels (< 63.695 ng/mL). In contrast, in patients with a mixed phenotype with hyperinflammation, those with high serum resistin levels (≥ 107.64 ng/mL) had a higher survival rate compared to those with lower resistin levels (< 107.64 ng/mL).
Discussion: Sepsis, the leading cause of death in intensive care unit patients. Identifying reliable biomarkers is essential for improving both the diagnosis and treatment of sepsis. We found that serum S100A8/A9 concentration at ICU admission is a significant predictor of 28-day mortality risk in sepsis patients. Additionally, resistin levels at ICU admission play an important role in predicting 28-day mortality risk in patients with both normal and mixed phenotypes with hyperinflammation. These findings suggest that S100A8/A9 and resistin could serve as effective biomarkers. Moreover, these findings could guide early clinical decisions in the treatment of sepsis patients.
Keywords: 28-day mortality; S100A8/A9; biomarkers; immunophenotype; resistin; sepsis.
Copyright © 2025 Chen, Liu, Zhou, Sun, Jiang and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comparison of total calprotectin levels with S100A8 and S100A9 subunit levels in critically ill patients.Scand J Clin Lab Invest. 2025;85(4):299-304. doi: 10.1080/00365513.2025.2512997. Epub 2025 Jun 2. Scand J Clin Lab Invest. 2025. PMID: 40455718
-
Serum Ferritin Levels as a Prognostic Marker for Predicting Outcomes in Children With Severe Sepsis and Their Correlation With Pediatric Sequential Organ Failure Assessment Score.Cureus. 2025 May 19;17(5):e84436. doi: 10.7759/cureus.84436. eCollection 2025 May. Cureus. 2025. PMID: 40539133 Free PMC article.
-
[Predictive value of plasma exosome count for the prognosis in septic patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Jul;36(7):687-692. doi: 10.3760/cma.j.cn121430-20230717-00529. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 39223881 Chinese.
-
Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD012404. doi: 10.1002/14651858.CD012404.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938790 Free PMC article.
-
Early intervention (mobilization or active exercise) for critically ill adults in the intensive care unit.Cochrane Database Syst Rev. 2018 Mar 27;3(3):CD010754. doi: 10.1002/14651858.CD010754.pub2. Cochrane Database Syst Rev. 2018. PMID: 29582429 Free PMC article.
Cited by
-
LILRA5+ macrophages drive early oxidative stress surge in sepsis: a single-cell transcriptomic landscape with therapeutic implications.Front Cell Infect Microbiol. 2025 Jul 28;15:1606401. doi: 10.3389/fcimb.2025.1606401. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40792106 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous