

Prognostic significance of unintentional weight loss in heart failure with preserved ejection fraction
- PMID: 40569185
- PMCID: PMC12292023
- DOI: 10.1002/ejhf.3745
Prognostic significance of unintentional weight loss in heart failure with preserved ejection fraction
Abstract
Aims: While intentional weight loss achieved through cardiometabolic medications has been associated with robust salutary effects in heart failure (HF) with preserved ejection fraction (HFpEF), the clinical significance of unintentional weight loss in this setting remains unclear.
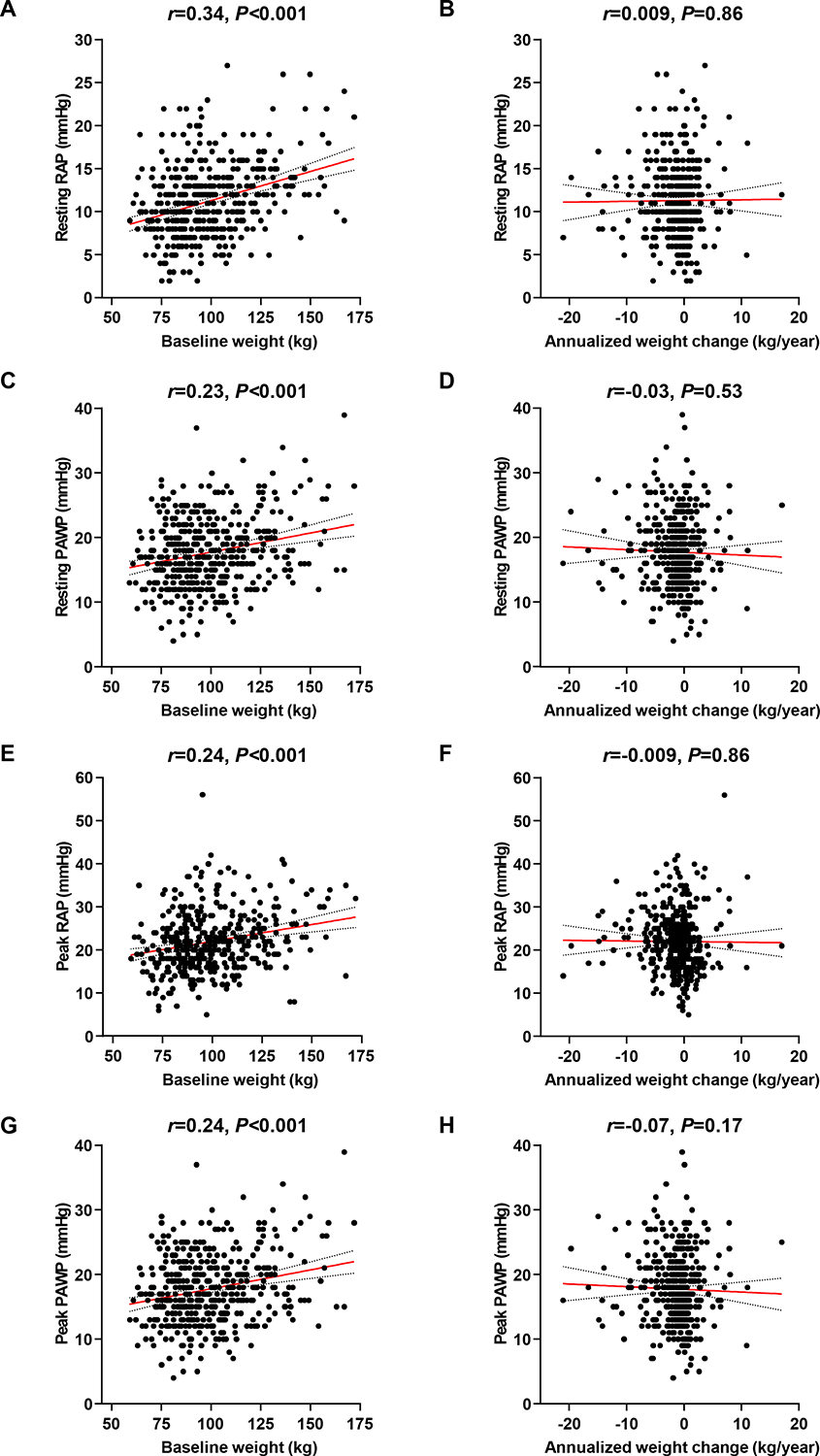
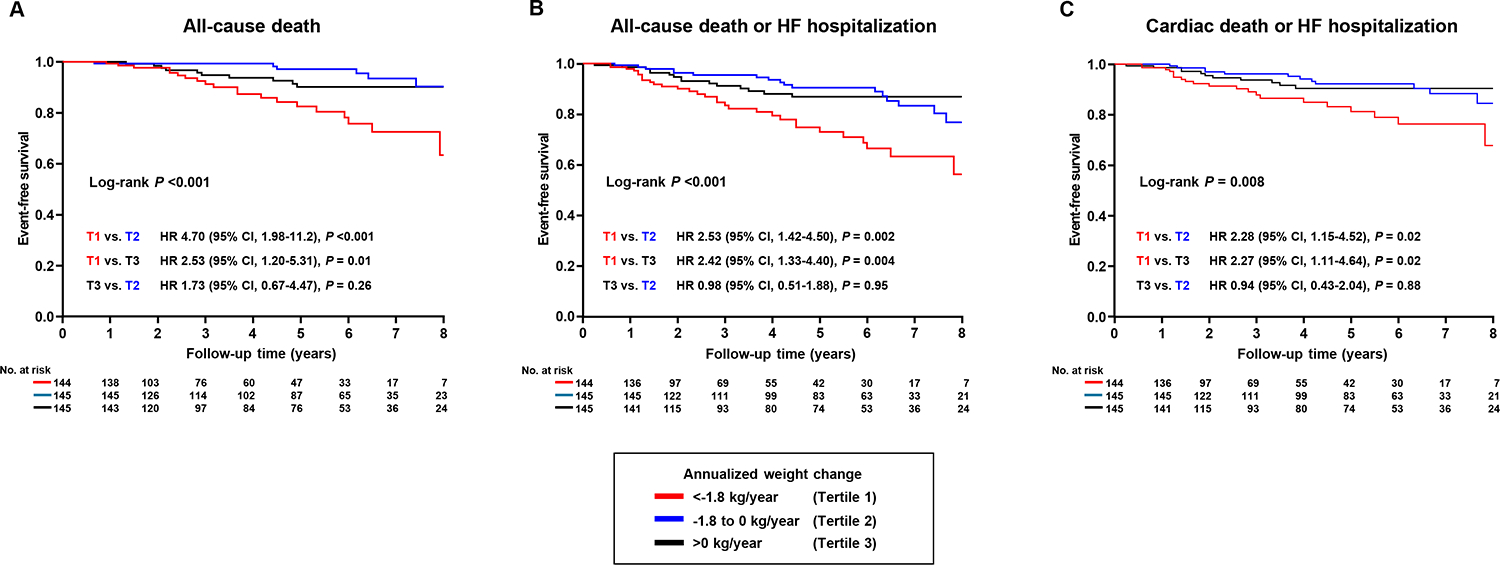
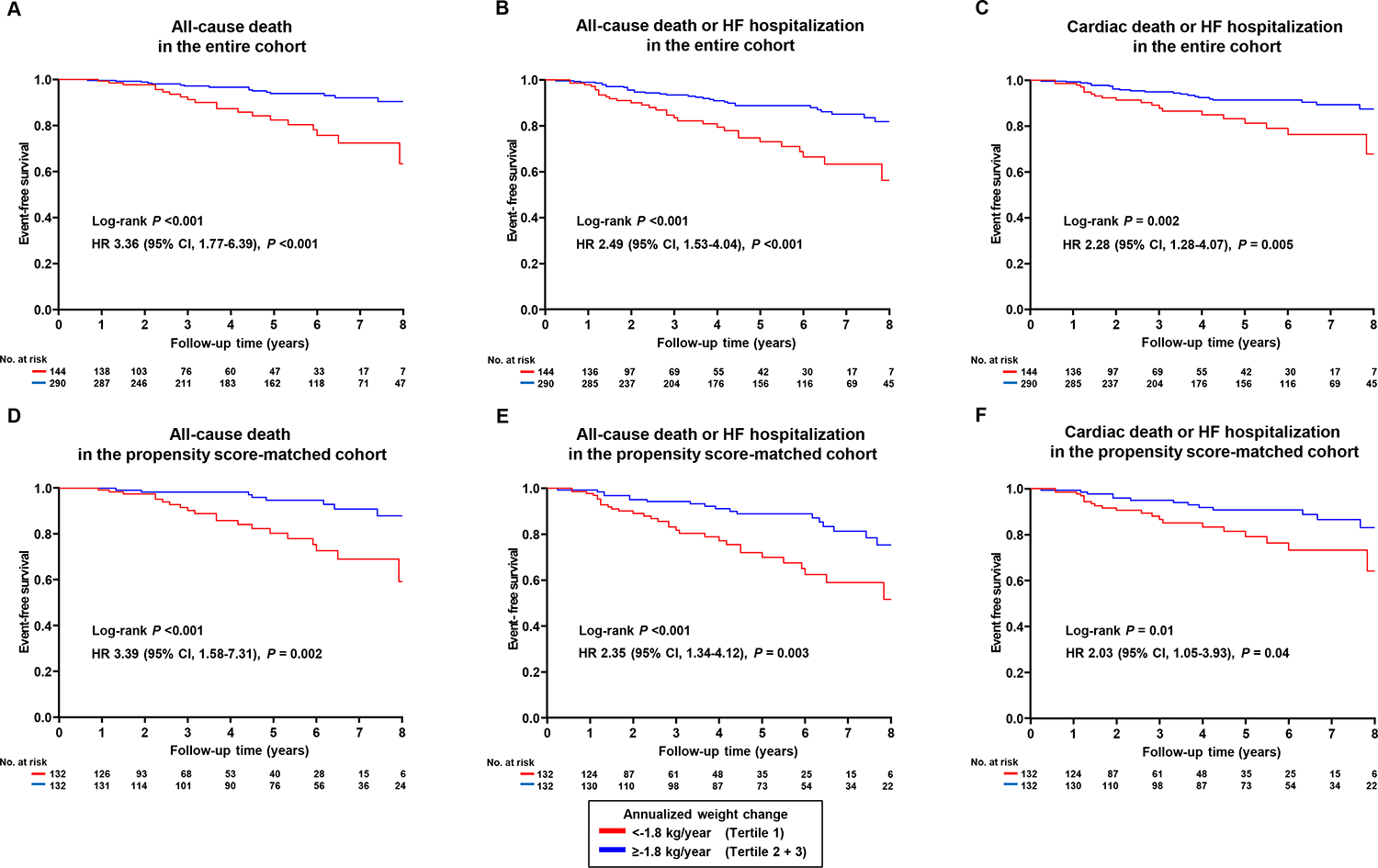
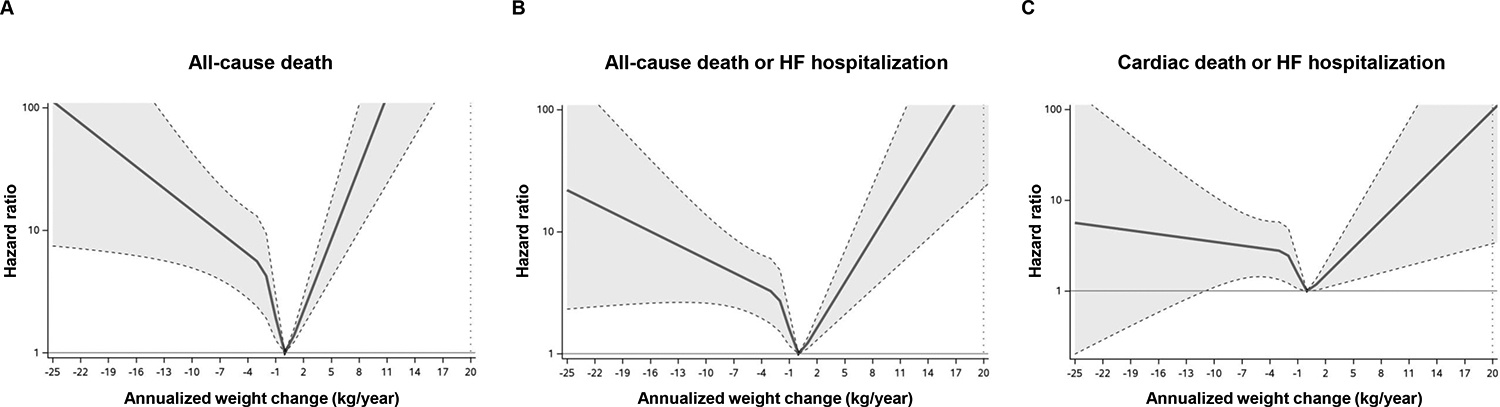
Methods and results: This retrospective cohort study included 434 overweight or obese patients with invasively proven HFpEF (67 ± 11 years, 236 female), without weight-reducing therapies or known malignancy, who underwent invasive hemodynamic cardiopulmonary testing and long-term clinical follow-up. The annualized weight change from index to final evaluation for the tertiles was: -21.1 to -1.8 kg/year (tertile 1); -1.8 to 0 kg/year (tertile 2); and 0 to +17.0 kg/year (tertile 3). Patients in tertile 1 had subtle abnormalities in ventilatory control at baseline, but there were no other significant differences between groups across a vast array of haemodynamic and metabolic parameters, both at rest and during exercise. Baseline weight was directly correlated with right and left heart filling pressures (r = 0.23-0.34, p < 0.001), but annualized weight change showed no correlation with any baseline haemodynamic measurements (all p > 0.05). Over a median follow-up of 4.7 years (interquartile range 2.3-6.5), patients in tertile 1 had higher risk of all-cause death (hazard ratio [HR] 3.36, 95% confidence interval [CI] 1.77-6.39, p < 0.001), all-cause death or HF hospitalization (HR 2.49, 95% CI 1.53-4.04, p < 0.001) and cardiac death or HF hospitalization (HR 2.28, 95% CI 1.28-4.07, p = 0.005) compared with those in tertile 2 or 3. These findings were consistent after multivariable adjustment.
Conclusions: Unintentional weight loss is associated with worse prognosis in patients with HFpEF and overweight or obesity, even as haemodynamics, exercise capacity, and gas exchange are not different from patients with stable or increasing weight. These data underline important and fundamental differences between therapeutic and unintended weight loss in HFpEF.
Keywords: Heart failure with preserved ejection fraction; Prognosis; Weight loss.
© 2025 European Society of Cardiology.
Figures
References
-
- Kosiborod MN, Deanfield J, Pratley R, Borlaug BA, Butler J, Davies MJ, et al. Semaglutide versus placebo in patients with heart failure and mildly reduced or preserved ejection fraction: a pooled analysis of the SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM randomised trials. Lancet 2024;404:949–961. 10.1016/S0140-6736(24)01643-X - DOI - PubMed
-
- Tada A, Burkhoff D, Naser JA, Harada T, Pourmussa B, Reddy YNV, et al. Dapagliflozin Enhances Arterial and Venous Compliance During Exercise in Heart Failure With Preserved Ejection Fraction: Insights From the CAMEO-DAPA Trial. Circulation 2024;150:997–1009. 10.1161/CIRCULATIONAHA.124.068788 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
