

Community health workers identify children requiring health center admission in Northern Uganda: prehospital risk prediction using vital signs and advanced point-of-care tests
- PMID: 40569209
- PMCID: PMC12203686
- DOI: 10.1080/16549716.2025.2519704
Community health workers identify children requiring health center admission in Northern Uganda: prehospital risk prediction using vital signs and advanced point-of-care tests
Abstract
Background: Over five million children die annually from preventable and treatable illnesses. Most of these deaths occur in sub-Saharan Africa, predominantly in socioeconomically deprived regions. With nearly half of pediatric mortality occurring at the community level, serious illnesses must be detected early in the prehospital setting. The purpose of this 18-month, prospective, observational pilot study was to introduce the first use of the proinflammatory biomarker, CRP, in the prehospital setting to community health workers and to develop a prehospital predictive model to identify sick children requiring health center admission.
Methods: We recruited 636 children presenting to one of four community health worker teams who completed a prehospital evaluation and referred each child to the closest health center. The primary outcome for this study was admission at the health center for more than 24 h. We used logistic regression to quantify the area under the receiver operating characteristic curve (AUC).
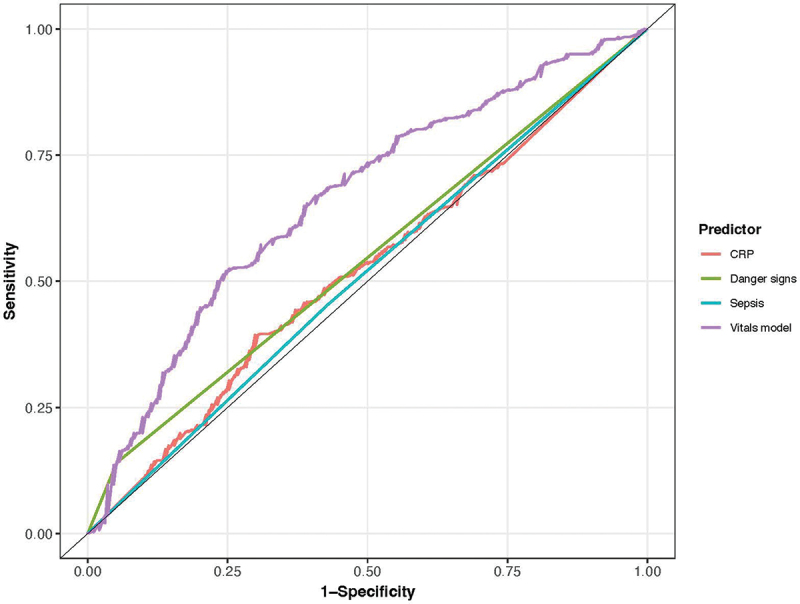
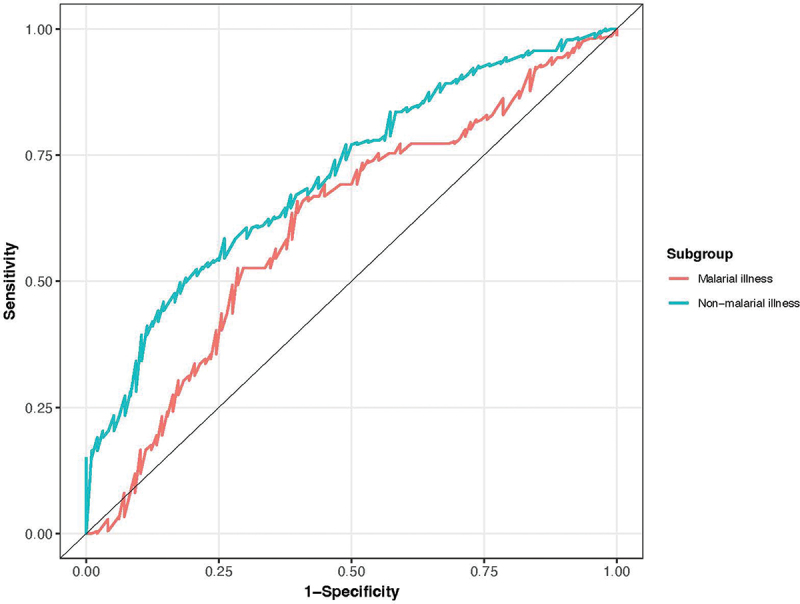
Results: We found poor discrimination of danger signs and CRP, with AUCs of 0.55 (95% CI 0.52-0.57) and 0.52 (95% CI 0.47-0.57), respectively. A model comprising vital signs demonstrated superior discrimination, with an AUC of 0.66 (95% CI 0.62-0.71), which improved with the addition of danger signs (AUC 0.69; 95% CI 0.64-0.73), and when restricted to children who tested negative for malaria (n = 327; AUC 0.71; 95% CI 0.65-0.77).
Conclusions: We demonstrate that performing advanced point-of-care tests is feasible in resource-limited community settings and present one of the first prehospital prediction models developed with community health workers.
Keywords: Community health worker; point-of-care tests; prehospital point-of-care; prehospital prediction; rapid diagnostic tests; seriously ill children; village health teams.
Plain language summary
Main Findings: Community health workers develop the first prehospital pediatric risk prediction model with advanced point-of-care testing.Added knowledge: Advanced point-of-care testing can be conducted by community health workers in prehospital settings; current standard of care for identifying seriously ill children has poor discrimination for hospital admission.Impact: A prehospital vital signs model demonstrates superior discrimination and can be expanded to create the first evidence-based risk prediction tool to identify seriously ill children at the community level.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- UNICEF . Levels and trends in child mortality. 2022.
-
- UDHS I . Uganda demographic and health survey. Kampala Uganda: Uganda Bureau of Statistics; 2011.
-
- Kane SS, Gerretsen B, Scherpbier R, et al. A realist synthesis of randomised control trials involving use of community health workers for delivering child health interventions in low and middle income countries. BMC Health Serv Res. 2010. Dec;10:1–7. doi: 10.1186/1472-6963-10-286 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous