

Receipt of Buprenorphine and Naltrexone for Opioid Use Disorder by Race and Ethnicity and Insurance Type
- PMID: 40569592
- PMCID: PMC12203278
- DOI: 10.1001/jamanetworkopen.2025.18493
Receipt of Buprenorphine and Naltrexone for Opioid Use Disorder by Race and Ethnicity and Insurance Type
Erratum in
-
Error in Abstract.JAMA Netw Open. 2025 Jul 1;8(7):e2527830. doi: 10.1001/jamanetworkopen.2025.27830. JAMA Netw Open. 2025. PMID: 40705339 Free PMC article. No abstract available.
Abstract
Importance: Despite expanded efforts to improve treatment access, inequities exist in the receipt of medications for opioid use disorder by race and ethnicity and insurance type.
Objective: To examine inequities in access to medications for opioid use disorder (MOUD)-specifically buprenorphine and naltrexone-by race and ethnicity and insurance type after opioid-related health care events.
Design, setting, and participants: This retrospective cohort study used data from the Institute for Health Equity Research Multi-Payor Claims Database, which includes more than 130 million individuals across commercial, Medicaid, and Medicare Advantage insurance plans. The cohort consisted of patients aged 18 years or older with an opioid use disorder (OUD)-related health care event (opioid-related overdose, infection, or treatment event) that occurred between January 1, 2017, and December 31, 2022. Statistical analysis was conducted from October 2023 to December 2024.
Exposure: Race and ethnicity and insurance type, including commercial insurance, Medicaid, and Medicare Advantage, were the primary exposures.
Main outcomes and measures: The primary outcome was receipt of MOUD (buprenorphine or naltrexone) within 180 days of an OUD-related health care event. Logistic regression models were used to assess the associations of MOUD receipt with race and ethnicity and with insurance type, adjusting for demographic, clinical, time, and geographical covariates.
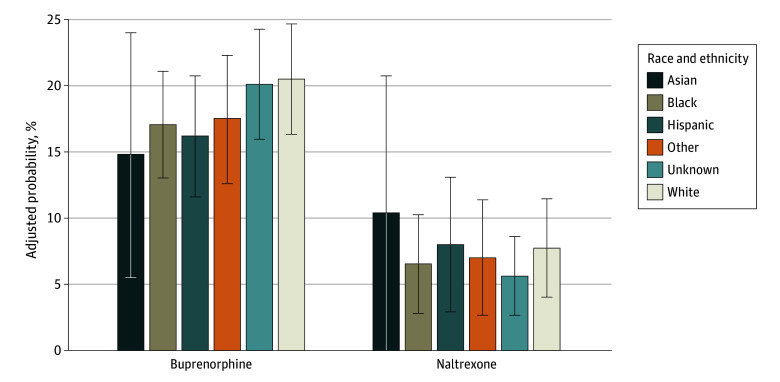
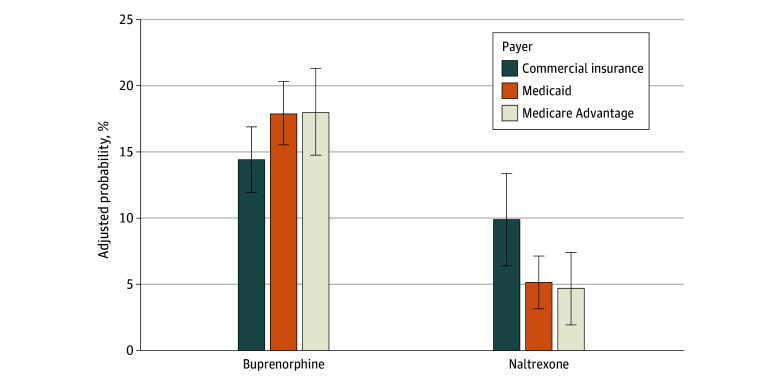
Results: Among 176 997 index events involving 164 728 patients between 2017 and 2022, the mean (SD) patient age was 40.0 (13.1) years; 104 005 (58.8%) involved men; 1083 events (0.6%) were among Asian patients, 23 424 (13.2%) were among Black patients, 10 302 (5.8%) were among Hispanic patients, 90 124 (50.9%) were among White patients, and 4697 (2.7%) were among patients of other race and ethnicity; and 147 257 (83.2%) were covered by Medicaid. Black (adjusted estimated probability, 17.1% [95% CI, 13.0%-21.1%]) and Hispanic (adjusted estimated probability, 16.2% [95% CI, 11.6%-20.8%]) patients were significantly less likely than White patients (adjusted estimated probability, 20.5% [95% CI, 16.4%-24.7%]) to receive buprenorphine (Black patients: adjusted odds ratio [AOR], 0.75 [95% CI, 0.63-0.90]; adjusted risk difference [ARD], -3.4 percentage points [pp] [95% CI, -6.5 to -0.4 pp]; Hispanic patients: AOR, 0.69 [95% CI, 0.51-0.92]; ARD, -4.4 pp [95% CI, -9.1 to 0.4 pp]) but received naltrexone at similar rates. Patients with Medicaid (AOR, 1.39 [95% CI, 1.14-1.69]; ARD, 3.5 pp [95% CI, 0.9-6.1 pp]) or Medicare Advantage (AOR, 1.40 [95% CI, 1.05-1.86]; ARD, 3.6 pp [95% CI, -0.6 to 7.7 pp]) were more likely to receive buprenorphine compared with those with commercial insurance. Buprenorphine access improved incrementally from 2017 to 2022, reflecting recent clinical and policy changes; however, disparities persisted.
Conclusions and relevance: In this cohort study of more than 17 600 opioid-related index health care events, race and ethnicity-based and insurance-based disparities in access to MOUD persisted despite efforts to expand treatment availability. These findings underscore the need for targeted interventions, including culturally tailored care, expanded access points, and policy reforms to address structural barriers and reduce inequities contributing to the overdose crisis.
Conflict of interest statement
Figures
References
-
- Spencer MR, Garnett MF, Miniño AM. Drug overdose deaths in the United States, 2002-2022. NCHS Data Briefs. 2024. Accessed September 4, 2024. https://www.cdc.gov/nchs/products/databriefs/db491.htm
-
- Hansen H, Roberts SK. Two tiers of biomedicalization: methadone, buprenorphine, and the racial politics of addiction treatment. In: Roberts SK, Netherland J, ed. Critical Perspectives on Addiction. Emerald Group Publishing Limited; 2012:79-102. doi: 10.1108/S1057-6290(2012)0000014008 - DOI
-
- Santo T Jr, Clark B, Hickman M, et al. Association of opioid agonist treatment with all-cause mortality and specific causes of death among people with opioid dependence: a systematic review and meta-analysis. JAMA Psychiatry. 2021;78(9):979-993. doi: 10.1001/jamapsychiatry.2021.0976 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
