

Uptake and patterns of PEP use within the context of a dynamic choice HIV prevention model in rural Uganda and Kenya: SEARCH Study
- PMID: 40569865
- PMCID: PMC12231643
- DOI: 10.1002/jia2.26450
Uptake and patterns of PEP use within the context of a dynamic choice HIV prevention model in rural Uganda and Kenya: SEARCH Study
Abstract
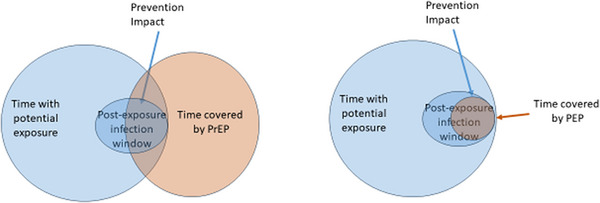
Introduction: Post-exposure prophylaxis (PEP) remains underutilized despite being the only prevention option currently available that covers risk after an exposure. We sought to evaluate uptake and patterns of use of PEP among men and women in rural Uganda and Kenya.
Methods: We analysed PEP uptake from three randomized trials enrolling persons aged ≥15 years with HIV risk from antenatal clinics, outpatient departments and community settings from April through August 2021 (NCT04810650). In each trial, participants were randomized to a person-centred, dynamic choice HIV prevention (DCP) model or standard-of-care (SoC) arm. DCP offered choice of biomedical product (oral pre-exposure prophylaxis [PrEP] or PEP) with an option to switch over time; service location (clinic vs. out-of-clinic); testing option (rapid blood-based test or oral HIV self-test). The SoC offered HIV prevention services as per in-country guidelines. In both arms, PEP comprised a 28-day oral Tenofovir/Lamivudine/Dolutegravir course with HIV testing at start and end of the 28-day period. We described patterns of and predictors of self-reported PEP use over the 12 months of follow-up.
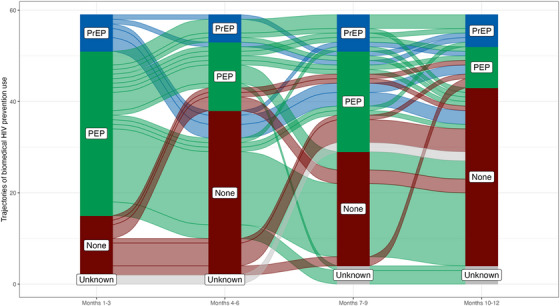
Results: A total of 1232 participants were enrolled, balanced by arm and country. Of the 1147 (93%) who completed at least one survey on self-reported use of biomedical prevention, the median follow-up time was 12 months [IQR: 11, 12]. Overall, a total of 104 courses of PEP were dispensed to 59 participants. PEP use was significantly higher among persons enrolled in the DCP arm (relative risk [RR] = 3.30; 95% CI: 1.58-6.91), from Uganda (RR = 3.17; 95% CI: 1.53-6.59), reporting alcohol use (RR = 2.20; 95% CI: 1.30-3.72) and men (RR = 2.08; 95% CI: 1.11-3.91). Of the 59 PEP users, 14 (24%) transitioned to PrEP and 28(47%) used PEP on more than one occasion. Multiple uses of PEP were more common among persons from Uganda versus Kenya (RR = 4.43; 95% CI: 1.10-17.80) and persons enrolled from the community (RR = 4.45; 95% CI: 1.89-10.45) versus clinic. There were no seroconversions reported among PEP users. No serious adverse events were reported.
Conclusions: PEP reaches groups such as men and those who use alcohol who are more likely to benefit from this short-term prevention modality than PrEP. There is a need to make PEP accessible within a context of person-centred delivery to optimize its benefits.
Keywords: HIV prevention; biomedical prevention; choice; person‐centred; post‐exposure prophylaxis; prevention coverage.
© 2025 The Author(s). Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of International AIDS Society.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Joint United Nations Programme on HIV/AIDS . Understanding Fast‐Track: accelerating action to end the AIDS epidemic by 2030. 2015. (Accessed September 16, 2024.) unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_F....
-
- https://www.who.int/teams/global‐hiv‐hepatitis‐and‐stis‐programmes/hiv/p... (Accessed 16 Sept 2024).
-
- UNAIDS . Global HIV & AIDS Statistics‐Fact Sheet. 2024. https://www.unaids.org/en/resources/fact‐sheet (Accessed 16 Sept 2024).
-
- Landovitz RJ, Hanscom BS, Clement ME, Tran HV, Kallas EG, Magnus M, et al. Efficacy and safety of long‐acting cabotegravir compared with daily oral tenofovir disoproxil fumarate plus emtricitabine to prevent HIV infection in cisgender men and transgender women who have sex with men 1 year after study unblinding: a secondary analysis of the phase 2b and 3 HPTN 083 randomised controlled trial. Lancet HIV. 2023;10(12):e767–e778. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
