

Hepatocyte Growth Factor: A Marker of Cardiac Function, Mortality, and Disease Subtype in Cardiac Amyloidosis
- PMID: 40570404
- PMCID: PMC12287948
- DOI: 10.1016/j.jacadv.2025.101828
Hepatocyte Growth Factor: A Marker of Cardiac Function, Mortality, and Disease Subtype in Cardiac Amyloidosis
Abstract
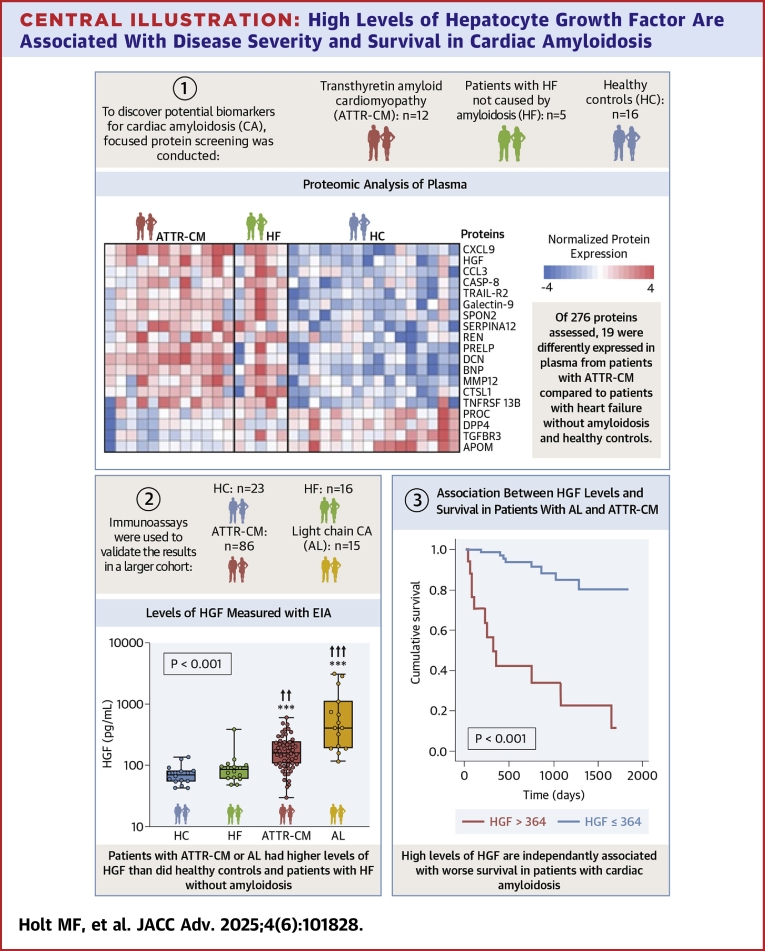
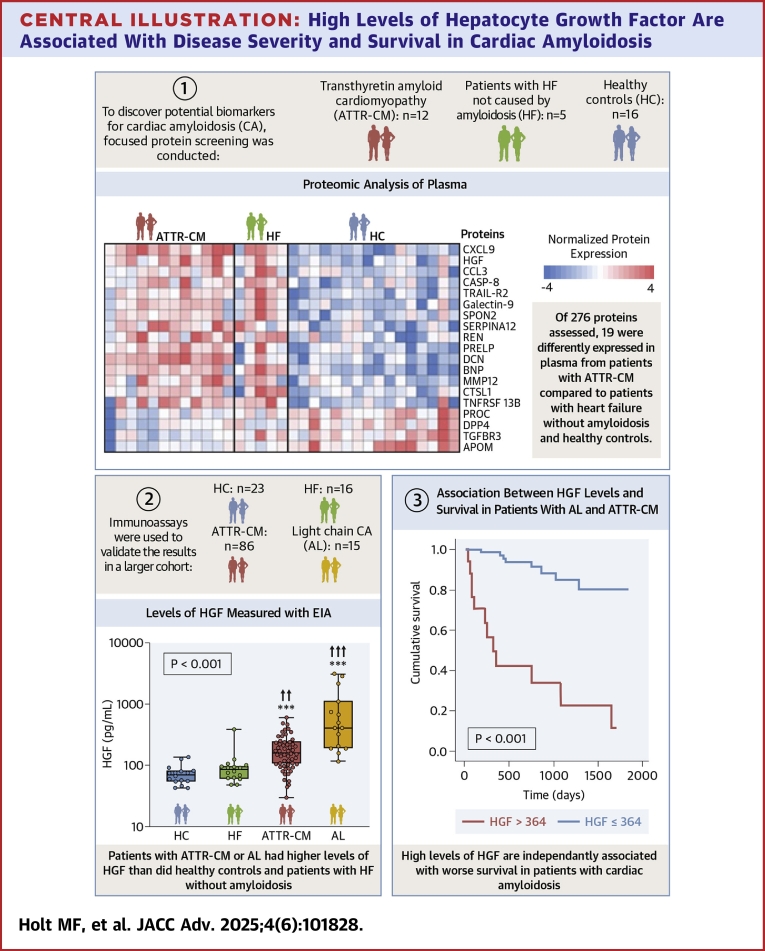
Background: It is important to reduce diagnostic delays for patients with cardiac amyloidosis (CA). Plasma biomarkers could streamline the diagnostic process and enhance prognostic accuracy.
Objectives: The authors aimed to identify circulating biomarkers capable of differentiating patients with CA from patients with heart failure (HF) and no amyloidosis. Additionally, we assessed whether these markers were associated with patient outcomes.
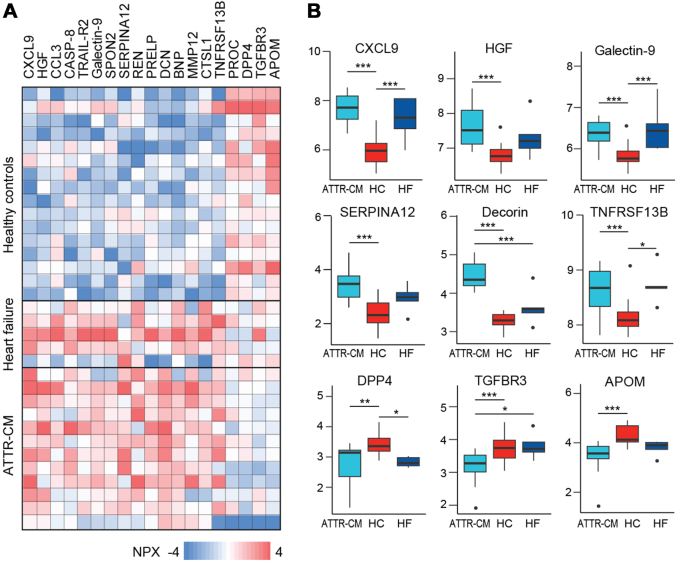
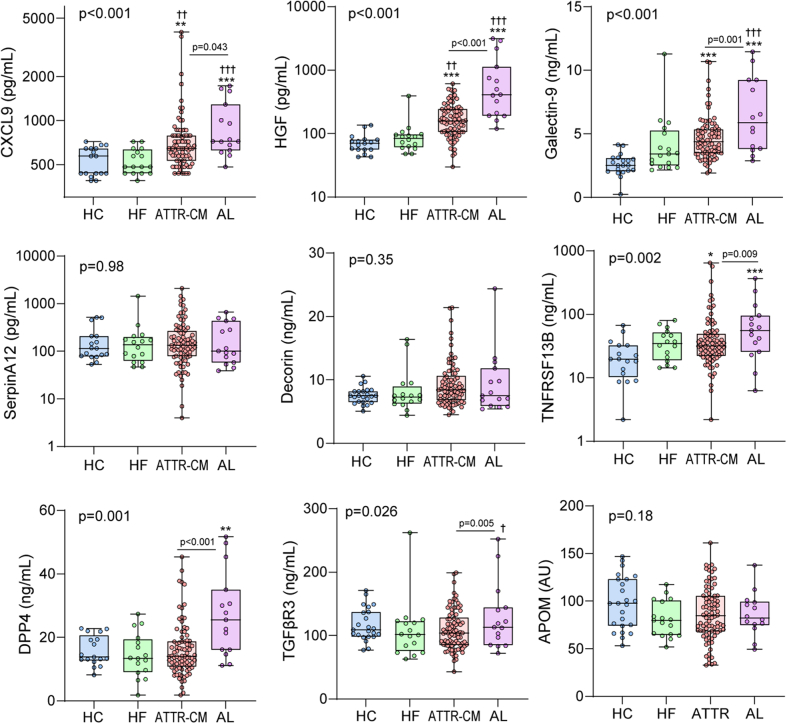
Methods: We performed focused protein screening in 12 patients with transthyretin CA, 5 patients with HF, and 16 healthy controls (HCs). To validate the findings, we used immunoassays to measure levels of differentially regulated proteins in a larger sample of 86 patients with transthyretin CA, 15 patients with light-chain CA, 16 patients with HF, and HCs. We compared protein levels between groups using multivariable general linear models. Associations between protein levels and all-cause mortality were assessed by receiver operating characteristic analysis.
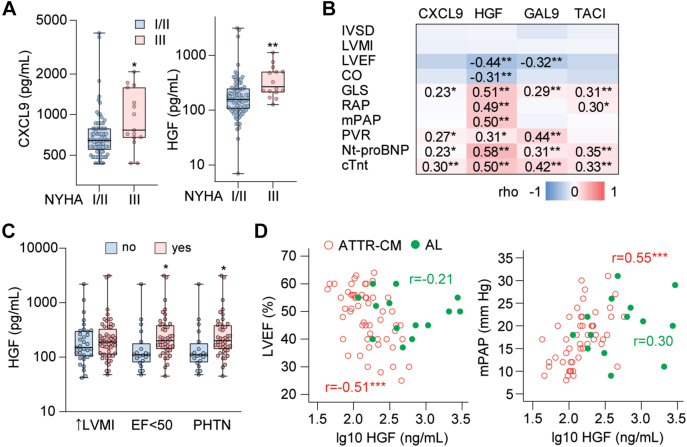
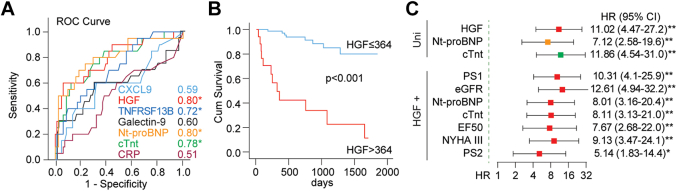
Results: We identified 99 candidate proteins by proteomic screening. In the validation sample, 4 of these markers were higher in CA than in HCs. Levels of C-X-C motif chemokine ligand 9 and hepatocyte growth factor (HGF) were also higher in CA than in HF. HGF correlated with measures of cardiac function in patients with transthyretin and light chain CA. HGF had a good discriminatory ability for predicting all-cause mortality (area under the curve = 0.80, P < 0.001), similar to those of N-terminal pro-B-type natriuretic peptide and troponin T.
Conclusions: Plasma HGF is a promising screening tool for CA. Higher levels of HGF are associated with more severe HF and worse prognosis in patients with CA.
Keywords: ATTR-CM; amyloid light chain; biomarker; cardiac amyloidosis; hepatocyte growth factor.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures The study was in part funded by a grant from The Bergesen Foundation and by a grant from The Blix Family Foundation to Dr Flesvig Holt. The study was in part funded by an unrestricted grant from Pfizer to Dr Gude. The study was in part funded by the K.G. Jebsen Centre for Cardiac Research. The funders were not involved in the collection, analysis, or interpretation of data; the writing of this article; or the decision to submit it for publication. Dr Gullestad has received lecture fees from AstraZeneca, Boehringer Ingelheim, and Novartis and has sat on advisory boards for AstraZeneca and Boehringer Ingelheim. Dr Broch has received lecture fees and consulting fees from Pfizer and has sat on advisory boards for AstraZeneca, Pharmacosmos, Boehringer Ingelheim, and Pfizer. Dr Gude has received grants and honoraria for lectures from Pfizer, Boehringer Ingelheim, and Novartis and has sat on advisory boards for Pfizer. Dr Wien has received lecture fees from Pfizer and Janssen-Cilag and has sat on advisory boards for Alnylam. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Plasma and cerebrospinal fluid amyloid beta for the diagnosis of Alzheimer's disease dementia and other dementias in people with mild cognitive impairment (MCI).Cochrane Database Syst Rev. 2014 Jun 10;2014(6):CD008782. doi: 10.1002/14651858.CD008782.pub4. Cochrane Database Syst Rev. 2014. PMID: 24913723 Free PMC article.
-
A New Measure of Quantified Social Health Is Associated With Levels of Discomfort, Capability, and Mental and General Health Among Patients Seeking Musculoskeletal Specialty Care.Clin Orthop Relat Res. 2025 Apr 1;483(4):647-663. doi: 10.1097/CORR.0000000000003394. Epub 2025 Feb 5. Clin Orthop Relat Res. 2025. PMID: 39915110
-
Are Current Survival Prediction Tools Useful When Treating Subsequent Skeletal-related Events From Bone Metastases?Clin Orthop Relat Res. 2024 Sep 1;482(9):1710-1721. doi: 10.1097/CORR.0000000000003030. Epub 2024 Mar 22. Clin Orthop Relat Res. 2024. PMID: 38517402
References
-
- Fontana M., Ćorović A., Scully P., Moon J.C. Myocardial amyloidosis: the exemplar interstitial disease. JACC Cardiovasc Imaging. 2019;12:2345–2356. - PubMed
-
- Merlini G., Westermark P. The systemic amyloidoses: clearer understanding of the molecular mechanisms offers hope for more effective therapies. J Intern Med. 2004;255:159–178. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
