

Neurally adjusted ventilatory assisted ventilation compared to pressure support during post-operative weaning of hepatic patients undergoing major abdominal surgeries: a randomized control trial
- PMID: 40571916
- PMCID: PMC12199501
- DOI: 10.1186/s12871-025-03159-y
Neurally adjusted ventilatory assisted ventilation compared to pressure support during post-operative weaning of hepatic patients undergoing major abdominal surgeries: a randomized control trial
Abstract
Objective: Patient-ventilator asynchrony (PVA) is a discrepancy between the patient’s demands and the ventilator. Pressure support ventilation (PSV) is the most popular mode of partial ventilation. Neurally adjusted ventilatory assist (NAVA) tailors the level of assistance to the diaphragm’s electromyographic activity. We aimed to evaluate the PVA during NAVA versus PSV in hepatic patients undergoing Whipple operation.
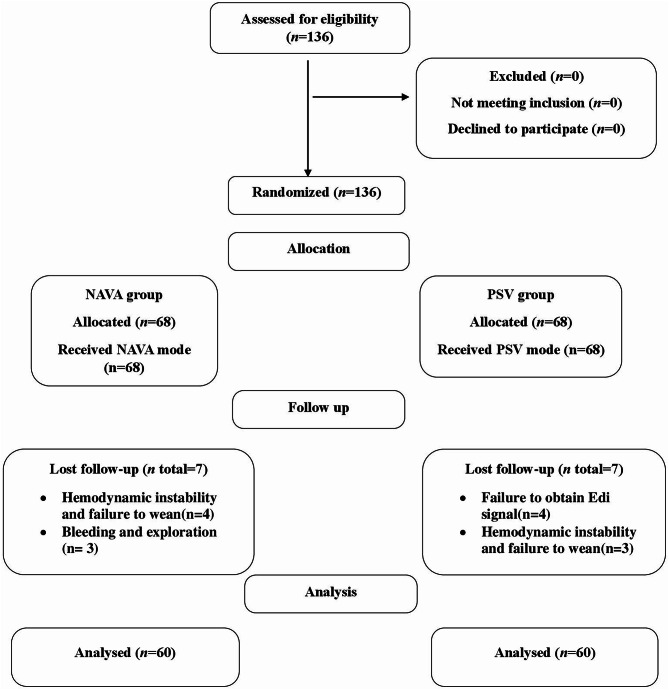
Methods: This study was a prospective, randomized, controlled double-blind trial. 120 adult Child-Pugh A and B hepatic patients of both sexes aged 18 to 65 years, undergoing Whipple operation, completed the study. We excluded severely debilitated patients and contraindications to the placement of the NAVA probe. 60 patients in the PSV (group) received PSV weaning mode, and 60 in the NAVA (group) received NAVA weaning mode. Outcome measures were asynchrony index, duration of mechanical ventilation MV, application and duration of post-extubation non-invasive CPAP, total sedating drug doses used, and ICU stay.
Results: The total asynchrony index was lower in the NAVA group than the PSV group, 6.12 ± 1.51 and 7.06 ± 1.25%, respectively, P < 0.001(95%CI 0.43 to 1.44). Cases with total ASI ≥ 10% were lower in the NAVA group than the PSV group, 6 and 16, respectively, P 0.02.The NAVA group had better oxygenation than PSV group, PaO2 and PaO2/FiO2 ratios were 208.53 ± 14.61 vs. 188.8 ± 25.55 mmHg, p < 0.001(95%CI -27.25 to -12.20) and 521.32 ± 36.52 vs. 472.01 ± 63.88, p < 0.001 (95%CI -68.12 to -30.50) respectively. The NAVA group had a lower duration of MV (4.05 ± 0.29 vs. 4.62 ± 0.52 h; P < 0.001(95%CI 0.41 to 0.72), auto-PEEP occurrence, and total doses of fentanyl and propofol than the PSV group.
Conclusions: NAVA serves better patient-ventilator interaction and synchronization than PSV, as indicated by a lower total asynchrony index, a reduced number of patients with total ASI ≥ 10%, the total doses of sedation used, the duration of MV needed, minimized need for post-extubation CPAP, and better oxygenation.
Trial registration: Menoufia University Faculty of Medicine research ethics committee IRB (N. and date 3/2020/ANET9), and National Liver Institute Menoufia University Institutional Review Board (NLI IRB 000140140). The study was retrospectively registered at the Pan African Clinical Trial with identification number PACTR202401894086611 on 26 January 2024.
Clinical registration: The study was registered at the Pan African Clinical Trial with identification number PACTR202401894086611.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12871-025-03159-y.
Keywords: Neurally adjusted ventilatory assist; Patient-ventilator asynchrony; Pressure support ventilation.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Local Menoufia university faculty of medicine research ethics committee IRB (N. and date 3/2020/ANET9), and National Liver Institute – Menoufia University Institutional Review Board (NLI IRB 000140140). Written informed consent was obtained from all participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Neurally Adjusted Ventilatory Assist versus Pressure Support Ventilation in Difficult Weaning: A Randomized Trial.Anesthesiology. 2020 Jun;132(6):1482-1493. doi: 10.1097/ALN.0000000000003207. Anesthesiology. 2020. PMID: 32217876 Clinical Trial.
-
Neurally adjusted ventilatory assist improves patient-ventilator interaction during postextubation prophylactic noninvasive ventilation.Crit Care Med. 2012 Jun;40(6):1738-44. doi: 10.1097/CCM.0b013e3182451f77. Crit Care Med. 2012. PMID: 22610179 Clinical Trial.
-
Patient-ventilator asynchrony during noninvasive pressure support ventilation and neurally adjusted ventilatory assist in infants and children.Pediatr Crit Care Med. 2013 Oct;14(8):e357-64. doi: 10.1097/PCC.0b013e3182917922. Pediatr Crit Care Med. 2013. PMID: 23863816 Clinical Trial.
-
Effect of Neurally Adjusted Ventilatory Assist on Patient-Ventilator Interaction in Mechanically Ventilated Adults: A Systematic Review and Meta-Analysis.Crit Care Med. 2019 Jul;47(7):e602-e609. doi: 10.1097/CCM.0000000000003719. Crit Care Med. 2019. PMID: 30882481
-
Neurally adjusted ventilatory assist as a weaning mode for adults with invasive mechanical ventilation: a systematic review and meta-analysis.Crit Care. 2021 Jun 29;25(1):222. doi: 10.1186/s13054-021-03644-z. Crit Care. 2021. PMID: 34187528 Free PMC article.
References
-
- Engelmann C, Clària J, Szabo G, Bosch J, Bernardi M. Pathophysiology of decompensated cirrhosis: Portal hypertension, circulatory dysfunction, inflammation, metabolism and mitochondrial dysfunction. J Hepatol. 2021;75 Suppl 1(Suppl 1):S49-S66. 10.1016/j.jhep.2021.01.002. PMID: 34039492; PMCID: PMC9272511. - PMC - PubMed
-
- Brackett DE, Sanghavi DK. Pressure Support. [Updated 2024 Jan 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. PMID: 31536312.
-
- Abramovitz A, Sung S, Pressure Support V. 2023 Jul 9. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31536312. - PubMed
-
- AK AK, Anjum F, Ventilator-Induced Lung Injury (VILI). 2023 Apr 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33085391. - PubMed
-
- Kyo M, Shimatani T, Hosokawa K, Taito S, Kataoka Y, Ohshimo S, Shime N. Patient-ventilator asynchrony, impact on clinical outcomes and effectiveness of interventions: a systematic review and meta-analysis. J Intensive Care. 2021;9(1):50. 10.1186/s40560-021-00565-5. PMID: 34399855; PMCID: PMC8365272. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
