

Point of care ultrasound assessment of the optic nerve sheath diameter in critically ill children
- PMID: 40571926
- PMCID: PMC12203719
- DOI: 10.1186/s12887-025-05798-z
Point of care ultrasound assessment of the optic nerve sheath diameter in critically ill children
Abstract
Background: Raised intracranial pressure (ICP) is a typical neurological problem in critically ill children, which is associated with poor clinical outcomes or even death. The purpose of the study was to evaluate the efficacy of optic nerve sheath diameter (ONSD) as a point-of-care testing in the pediatric intensive care units for early diagnosis of raised intracranial pressure and as a follow up tool for treatment response.
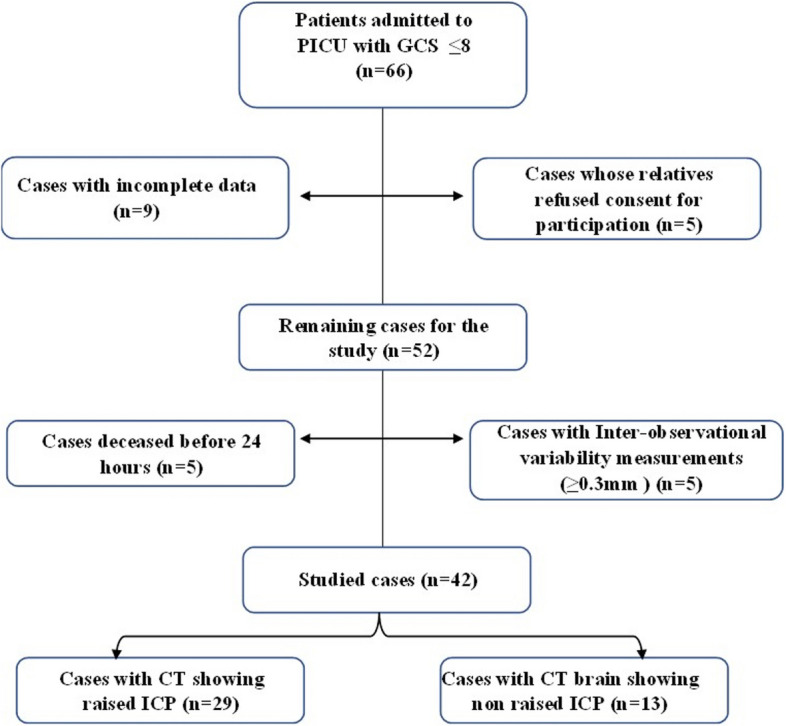
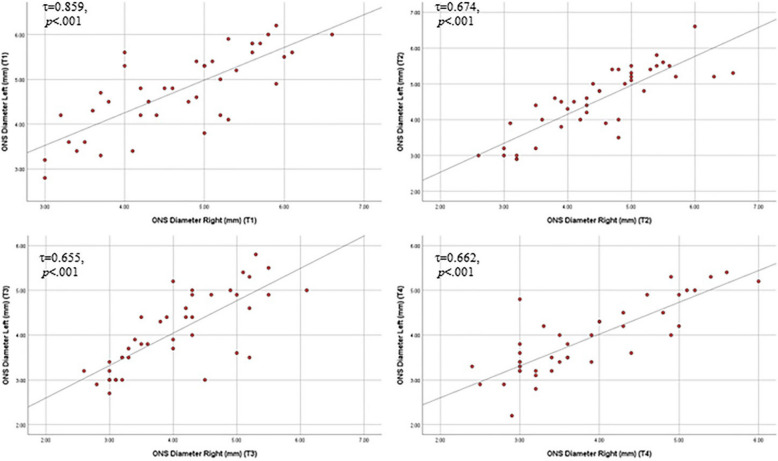
Method: A prospective observational study was conducted in the pediatric intensive care unit of a tertiary care children's hospital. Consecutive children aged one month to twelve years with Glasgow Coma Scale less than or equal to 8 were included. Brain CT was performed just before or within few hours of admission to identify raised ICP. Two trained examiners in the same work place, who were blinded to the clinical details of the patients, performed the ONSD sonography concurrently. The ONSD was measured in the left and right eyes on admission, after 1 h, after 12 h, and after 24 h.
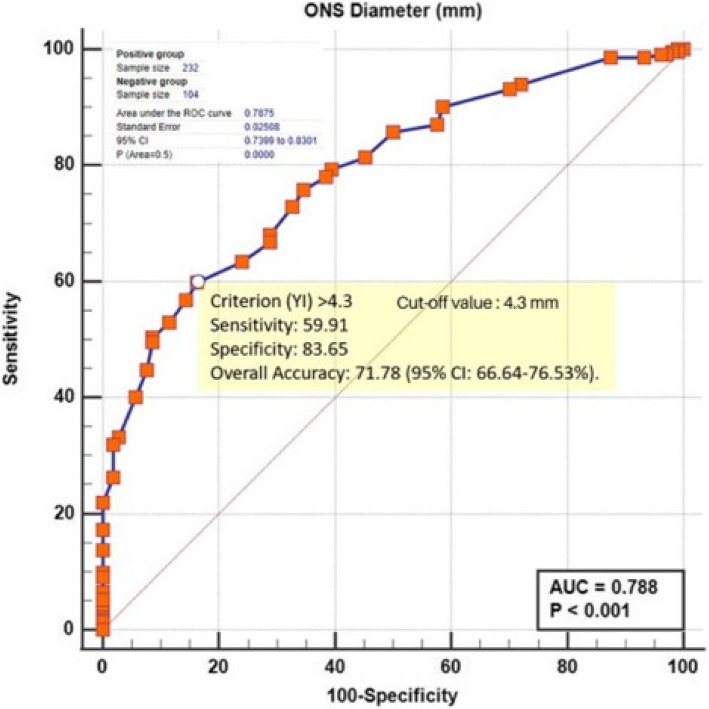
Results: Forty-two patients were categorized into 29 children with raised ICP and 13 children with non-raised ICP. The ONSD was significantly higher in the raised ICP group at all times in both eyes. It showed a significant decrease over time in both groups. A cutoff value of ≥ 4.3 mm was found to be an acceptable discriminator of ICP with Area Under the ROC curve (AUC) = 0.788 (95% CI 0.740- 0.830) (p < 0.0001), sensitivity of 59.91% (95% CI: 53.30-66.27) and specificity of 83.65% (95% CI: 75.12-90.18).
Conclusions: In critically ill children with non-traumatic causes of raised ICP, point of care ultrasound of ONSD shows a good diagnostic test accuracy for early diagnosis of raised ICP as well as follow up tool of treatment response if used serially. In addition, it is very good at correctly identifying individuals who do not have raised ICP to avoid unnecessary interventions.
Keywords: Critically ill children; Intensive care unit; Intracranial pressure; Non-invasive monitoring; Optic nerve sheath diameter; Point-of- care ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Alexandria University (IRB No: 00012098- FWA No: 00018699) on December 16 th, 2021; serial number: 0106996. Written informed consents were obtained from the patients'parents or legal guardians. Consent for publication: The authors affirm that informed consent for publication of the images in Fig. (1) was provided from patient's parents. Competing interests: The authors declare no competing interests.
Figures

References
-
- Freeman WD. Management of Intracranial Pressure [published correction appears in Continuum (Minneap, Minn) 2015. Dec;21 (6 Neuroinfectious Disease) :1550]. Continuum (Minneap Minn). 2015; 21 (5 Neurocritical Care):1299–1323. - PubMed
-
- Sankhyan N, Vykunta Raju KN, Sharma S, Gulati S. Management of raised intracranial pressure. Indian J Pediatr. 2010;77:1409–16. - PubMed
-
- Zhang X, Medow JE, Iskandar BJ, Wang F, Shokoueinejad M, Koueik J, et al. Invasive and noninvasive means of measuring intracranial pressure: a review. Physiol Meas. 2017;38:R143–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
