

Impact of Early MPO-ANCA Positivity on Unique Clinical Features in Korean Patients with EGPA: A Single-Centre Cohort Study
- PMID: 40572776
- PMCID: PMC12194988
- DOI: 10.3390/medicina61061088
Impact of Early MPO-ANCA Positivity on Unique Clinical Features in Korean Patients with EGPA: A Single-Centre Cohort Study
Abstract
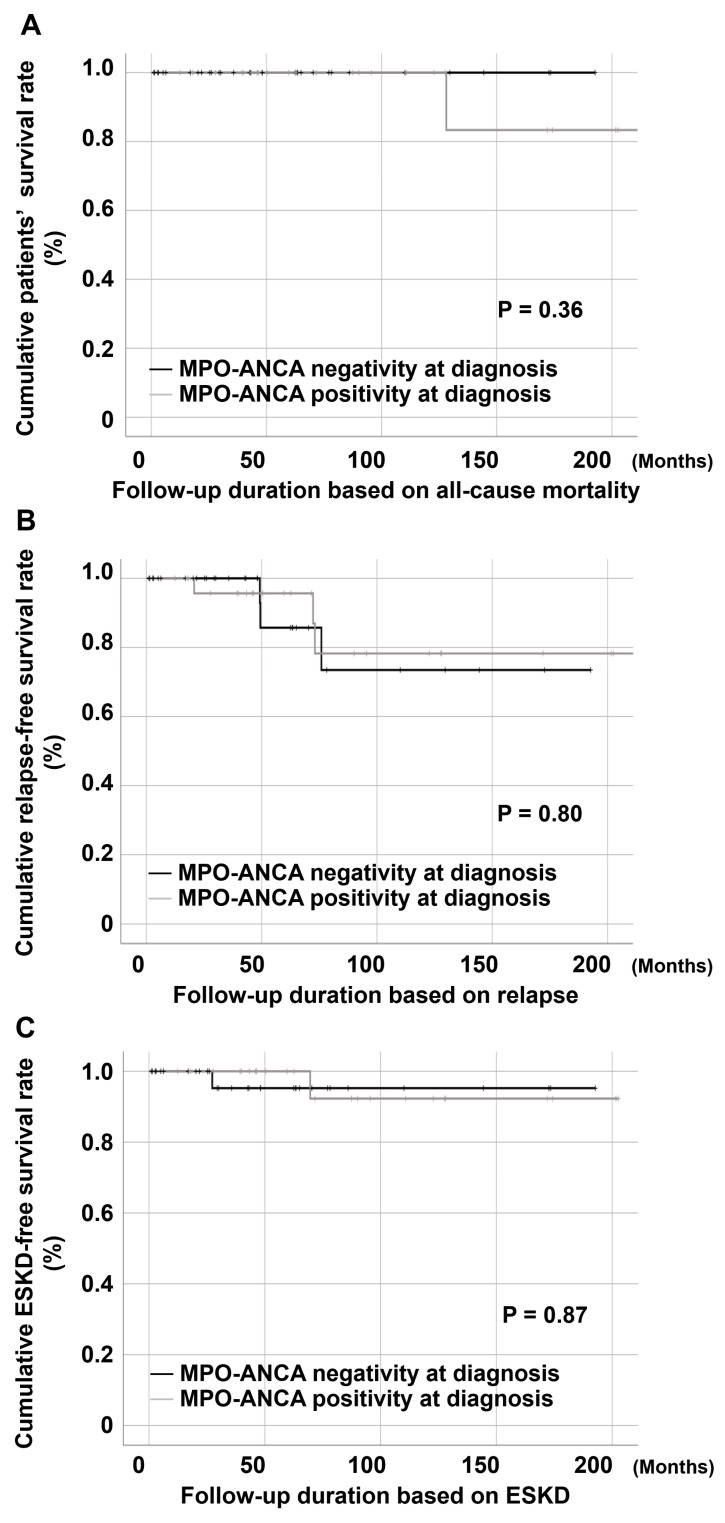
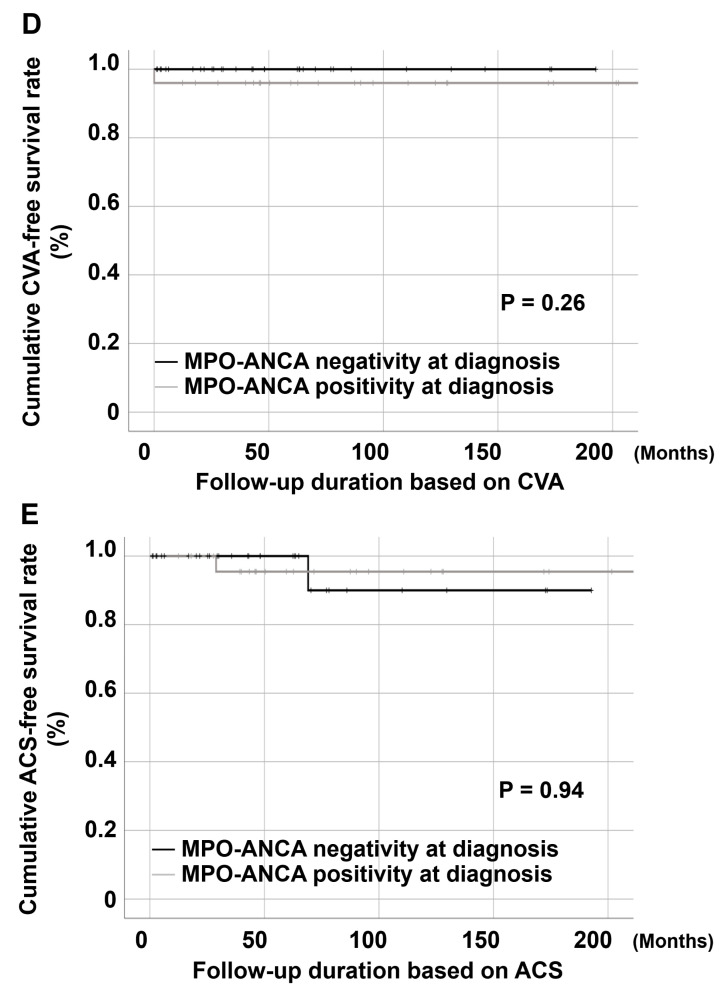
Objectives: Previous studies have suggested differences in vasculitic and eosinophilic phenotypes based on anti-neutrophil cytoplasmic antibody (ANCA) positivity in eosinophilic granulomatosis with polyangiitis (EGPA). However, their relevance under the 2022 American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) classification criteria remains unclear. We aimed to evaluate the clinical features and outcomes of EGPA according to myeloperoxidase (MPO)-ANCA status in a Korean cohort. Methods: We conducted a retrospective cohort study that included 57 patients with EGPA without proteinase 3-ANCA positivity who fulfilled the 2022 ACR/EULAR classification criteria. Patients were classified into MPO-ANCA-positive (n = 25) and MPO-ANCA-negative (n = 32) groups. Clinical manifestations, laboratory findings, and outcomes, including all-cause mortality, relapse, end-stage kidney disease (ESKD), cerebrovascular accident (CVA), and acute coronary syndrome (ACS), were compared between the two groups. Results: MPO-ANCA-positive patients exhibited higher Five-Factor Scores (1.0 [0.0-1.0] vs. 0.0 [0.0-1.0], p = 0.038), lower Short Form 36 Physical Component Summary scores (35.0 [19.7-56.3] vs. 52.5 [43.5-69.7], p = 0.048), and elevated systemic inflammation markers (higher erythrocyte sedimentation rate: 58.0 [16.0-97.5] mm/hr vs. 25.5 [7.0-63.8] mm/hr, p = 0.026). Constitutional symptoms were more frequent among MPO-ANCA-positive patients (n = 14 [56.0%] vs. n = 3 [9.4%], p < 0.001), whereas no significant differences were found in vasculitic or eosinophilic manifestations. Kaplan-Meier analysis revealed no differences in the overall (p = 0.36), relapse-free (p = 0.80), ESKD-free (p = 0.87), CVA-free (p = 0.26), or ACS-free (p = 0.94) survival rates between the two groups. Conclusions: In Korean patients with EGPA classified under the 2022 ACR/EULAR classification criteria, MPO-ANCA positivity, as compared to ANCA-negative status, was associated with a higher disease burden and poorer quality of life but not with distinct vasculitic or eosinophilic manifestations and adverse outcomes.
Keywords: anti-neutrophil cytoplasmic antibody; clinical; feature; myeloperoxidase; vasculitis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Jakes R.W., Kwon N., Nordstrom B., Goulding R., Fahrbach K., Tarpey J., Van Dyke M.K. Burden of illness associated with eosinophilic granulomatosis with polyangiitis: A systematic literature review and meta-analysis. Clin. Rheumatol. 2021;40:4829–4836. doi: 10.1007/s10067-021-05783-8. - DOI - PMC - PubMed
-
- Emmi G., Bettiol A., Gelain E., Bajema I.M., Berti A., Burns S., Cid M.C., Cohen Tervaert J.W., Cottin V., Durante E., et al. Evidence-based guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat. Rev. Rheumatol. 2023;19:378–393. doi: 10.1038/s41584-023-00958-w. - DOI - PubMed
-
- Comarmond C., Pagnoux C., Khellaf M., Cordier J.F., Hamidou M., Viallard J.F., Maurier F., Jouneau S., Bienvenu B., Puéchal X., et al. Eosinophilic granulomatosis with polyangiitis (churg-strauss): Clinical characteristics and long-term followup of the 383 patients enrolled in the french vasculitis study group cohort. Arthritis Rheum. 2013;65:270–281. doi: 10.1002/art.37721. - DOI - PubMed
-
- Sinico R.A., Di Toma L., Maggiore U., Bottero P., Radice A., Tosoni C., Grasselli C., Pavone L., Gregorini G., Monti S., et al. Prevalence and clinical significance of antineutrophil cytoplasmic antibodies in churg-strauss syndrome. Arthritis Rheum. 2005;52:2926–2935. doi: 10.1002/art.21250. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
