

Cold Atmospheric Plasma Improves the Therapeutic Success of Photodynamic Therapy on UV-B-Induced Squamous Cell Carcinoma in Hairless Mice
- PMID: 40573301
- PMCID: PMC12196468
- DOI: 10.3390/ph18060907
Cold Atmospheric Plasma Improves the Therapeutic Success of Photodynamic Therapy on UV-B-Induced Squamous Cell Carcinoma in Hairless Mice
Abstract
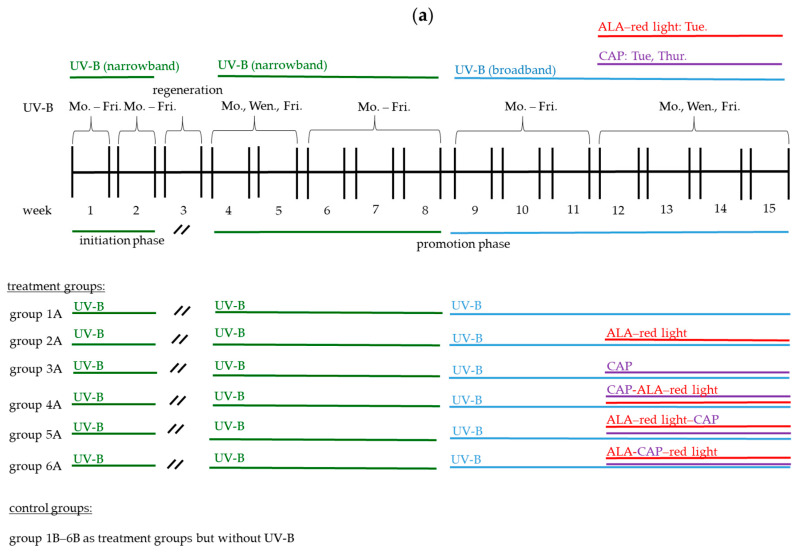
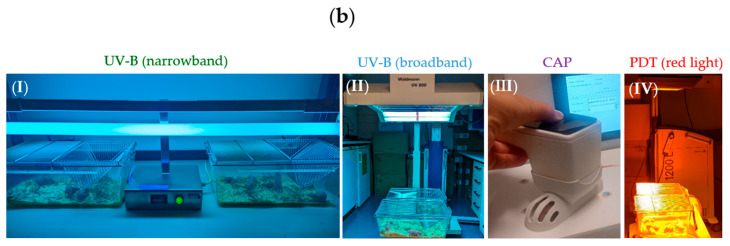
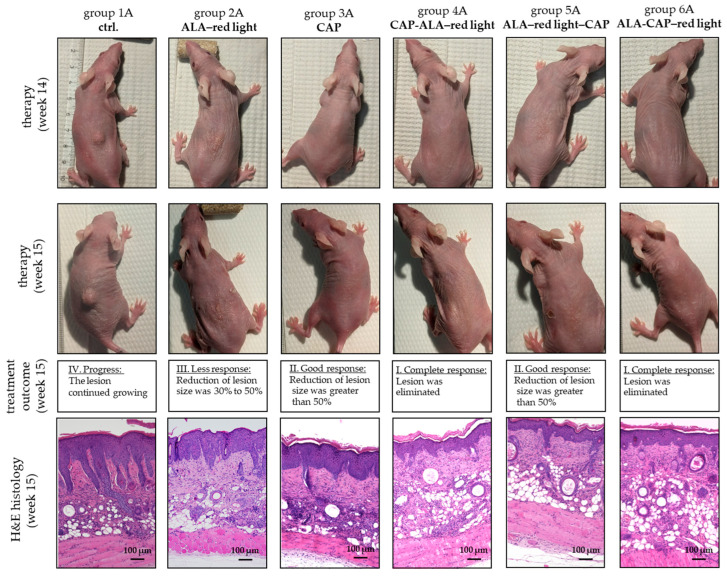
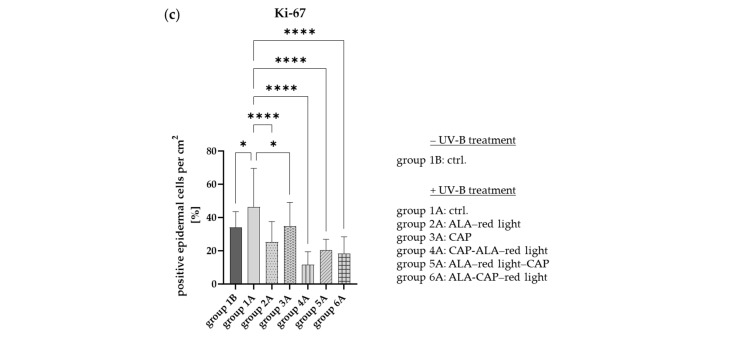
Background/Objectives: Actinic keratosis (AK) occurs on sun-damaged skin and is considered a precursor to squamous cell carcinoma (SCC). Photodynamic therapy (PDT), using 5-aminolevulinic acid (ALA) and red light, is a common treatment for AK. However, its clinical efficacy for invasive tumors such as SCC is limited by the poor penetration and distribution of the photosensitizer. Cold atmospheric plasma (CAP), a partially ionized gas, increases skin permeability and exhibits anti-cancer properties through the generation of reactive oxygen species (ROS). In a previous study, CAP showed promising synergistic effects when combined with ALA-PDT for the treatment of SCC cells in vitro. The present study investigated the effects of combining CAP with ALA-PDT on cutaneous AK and SCC induced by ultraviolet B (UV-B) irradiation in SKH1 hairless mice. Methods: We compared various application sequences (CAP-ALA-red light, ALA-red light-CAP, and ALA-CAP-red light) against conventional ALA-PDT using visual, histological, and molecular assessments of the affected skin. Results: The results demonstrated that combined treatments strongly inhibited the growth of UV-B-induced skin lesions. TUNEL staining revealed increased apoptosis following both single and combined therapies, while Ki-67 staining indicated reduced keratinocyte proliferation and diminished DNA damage in treated areas. mRNA expression analysis showed the upregulation of apoptosis-related genes (p16INK4a, p21CIP1) alongside enhanced anti-tumor immune responses (IL-6, IL-8) in the affected tissue samples. Notably, the combined treatment enhances the therapeutic effect, whereas the sequence of application does not seem to be relevant for therapeutic efficacy in vivo. Conclusions: Overall, these results suggest that CAP may enhance the anti-tumor effect of conventional ALA-PDT, supporting previous findings on SCC cells.
Keywords: 5-aminolaevulinic acid (ALA); actinic keratosis (AK); cold atmospheric plasma (CAP); photodynamic therapy (PDT); squamous cell carcinoma (SCC).
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures








References
-
- Kandolf L., Peris K., Malvehy J., Mosterd K., Heppt M.V., Fargnoli M.C., Berking C., Arenberger P., Bylaite-Bučinskiene M., Del Marmol V. European consensus-based interdisciplinary guideline for diagnosis, treatment and prevention of actinic keratoses, epithelial UV-induced dysplasia and field cancerization on behalf of European Association of Dermato-Oncology, European Dermatology Forum, European Academy of Dermatology and Venereology and Union of Medical Specialists (Union Européenne des Médecins Spécialistes) J. Eur. Acad. Dermatol. Venereol. 2024;38:1024–1047. - PubMed
-
- Green A.C., Soyer H., Prow T., Jemec G., editors. Epidemiology of actinic keratoses. Curr. Probl. Dermatol. 2014;46:1–7. - PubMed
-
- Agarwal K., Podder I., Cockerell C.J., Kassir M., Grabbe S., Goldust M. Update on diagnosis and treatment of actinic keratosis. Dermatol. Rev. 2022;3:359–368. doi: 10.1002/der2.121. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
