

A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition
- PMID: 40573553
- PMCID: PMC12196683
- DOI: 10.3390/s25123664
A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition
Abstract
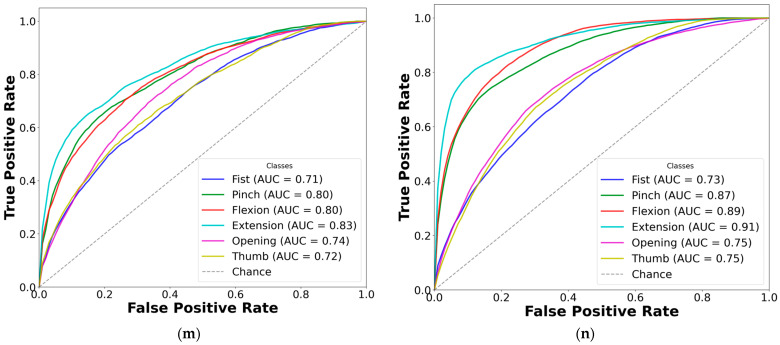
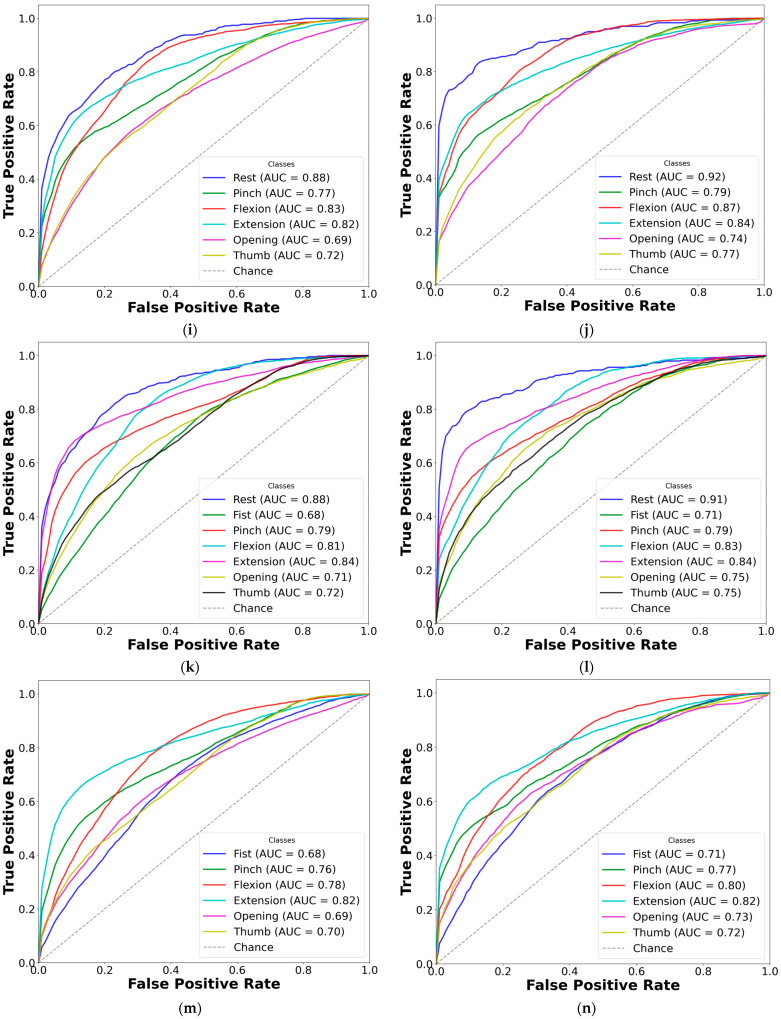
We introduce a hybrid deep learning model for recognizing hand gestures from electromyography (EMG) signals in subacute stroke patients: the one-dimensional convolutional long short-term memory neural network (CNN-LSTM). The proposed network was trained, tested, and cross-validated on seven hand gesture movements, collected via EMG from 25 patients exhibiting clinical features of paresis. EMG data from these patients were collected twice post-stroke, at least one week apart, and divided into datasets A and B to assess performance over time while balancing subject-specific content and minimizing training bias. Dataset A had a median post-stroke time of 16.0 ± 8.6 days, while dataset B had a median of 19.2 ± 13.7 days. In classification tests based on the number of gesture classes (ranging from two to seven), the hybrid model achieved accuracies ranging from 85.66% to 82.27% in dataset A and from 88.36% to 81.69% in dataset B. To address the limitations of deep learning with small datasets, we developed a novel bilateral data fusion approach that incorporates EMG signals from the non-paretic limb during training. This approach significantly enhanced model performance across both datasets, as evidenced by improvements in sensitivity, specificity, accuracy, and F1-score metrics. The most substantial gains were observed in the three-gesture subset, where classification accuracy increased from 73.01% to 78.42% in dataset A, and from 77.95% to 85.69% in dataset B. In conclusion, although these results may be slightly lower than those of traditional supervised learning algorithms, the combination of bilateral data fusion and the absence of feature engineering offers a novel perspective for neurorehabilitation, where every data segment is critically significant.
Keywords: CNN-LSTM; deep learning; electromyography (EMG); hand gesture recognition; healthcare; machine learning; neurorehabilitation; paresis; stroke; upper extremity motor impairment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures










References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
