

A Natural Latex-Based Smart Dressing for Curcumin Delivery Combined with LED Phototherapy in Diabetic Foot Ulcers: A Pilot Clinical Study
- PMID: 40574084
- PMCID: PMC12196574
- DOI: 10.3390/pharmaceutics17060772
A Natural Latex-Based Smart Dressing for Curcumin Delivery Combined with LED Phototherapy in Diabetic Foot Ulcers: A Pilot Clinical Study
Abstract
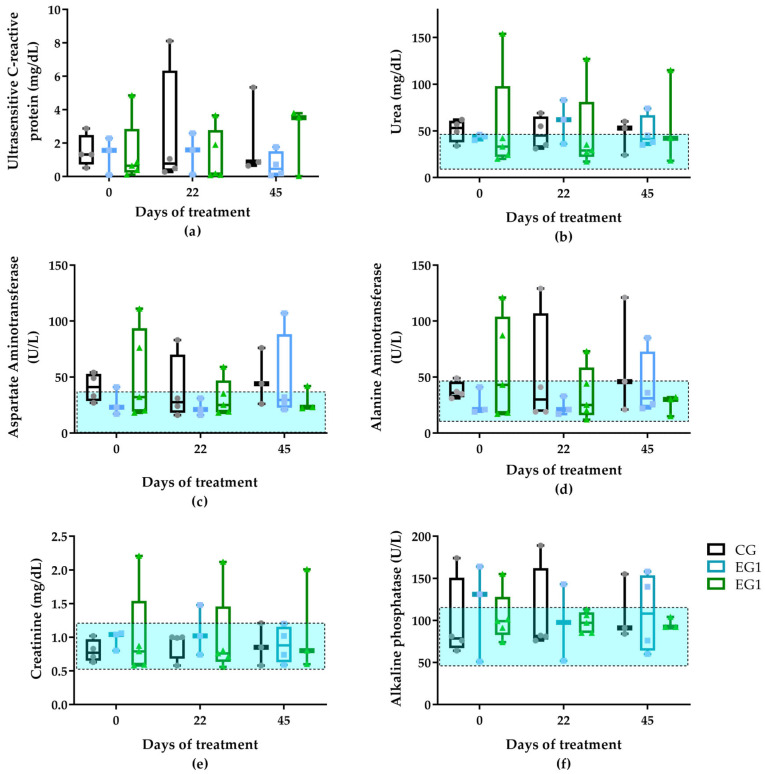
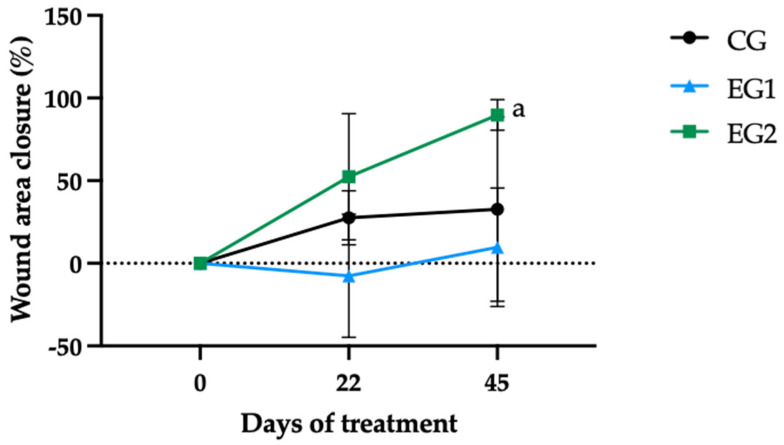
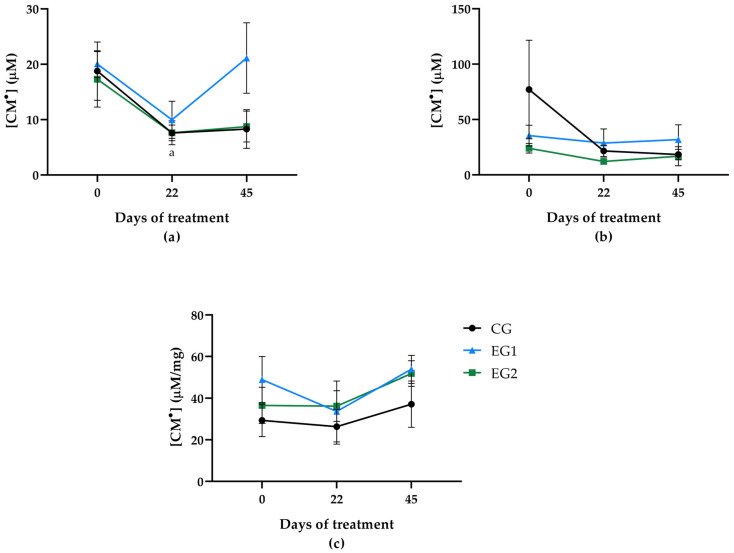
Background: Diabetic foot ulcers (DFUs) affect 25% of diabetes patients, with high risks of amputation (70%), recurrence (65% within 3-5 years), and mortality (50-70% at 5-years). Current treatments are limited by persistent inflammation, oxidative stress, and cost barriers. This study evaluates a bioactive dressing combining a natural latex-based (NLB) biomembrane (Hevea brasiliensis) with curcumin-loaded liposomes, exhibiting angiogenic and antimicrobial properties, and red LED (light-emitting diode) phototherapy (635-640 nm) to address these challenges. Methods: A pilot clinical trial randomized 15 DFU participants into three groups: Control (CG, n = 5, standard care); Experimental Group 1 (EG1, n = 5, NLB + LED, daily treatment); and Experimental Group 2 (EG2, n = 5, NLB-curcumin liposomes + LED, daily treatment). Outcomes included wound closure, inflammatory/oxidative markers, and therapy feasibility. Assessments at D0, D22, and D45 included hematological/biochemical profiling, reactive oxygen species (ROS), and wound area measures. Results: On day 45, GE2 showed an average ulcer contraction of 89.8%, while CG showed 32.8%, and GE1 showed 9.7%. Systemic ROS and biomarkers (C-reactive protein, leukocytes) showed no significant changes (p > 0.05), though transient inflammatory spikes occurred. The combined therapy (EG2) accelerated healing without direct biomarker correlations. Conclusions: These findings highlight the potential of this combined therapy as an accessible, cost-effective DFU treatment, warranting larger studies to optimize home-based protocols and elucidate mechanisms.
Keywords: clinical assay; curcumin; natural latex biomembrane; oxidative stress; ulcers; wound healing.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Borderie G., Foussard N., Larroumet A., Blanco L., Barbet-Massin M.-A., Ducos C., Rami-Arab L., Domenge F., Mohammedi K., Ducasse E., et al. The skin autofluorescence of advanced glycation end-products relates to the development of foot ulcers in type 2 diabetes: A longitudinal observational study. J. Diabetes Complicat. 2023;37:108595. doi: 10.1016/j.jdiacomp.2023.108595. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
