

Clinical manifestations of anxiety and depression in sepsis-associated encephalopathy and multi-omics identification of cluster of differentiation 38 as an early biomarker
- PMID: 40574780
- PMCID: PMC12188886
- DOI: 10.5498/wjp.v15.i6.105889
Clinical manifestations of anxiety and depression in sepsis-associated encephalopathy and multi-omics identification of cluster of differentiation 38 as an early biomarker
Abstract
Background: Sepsis-associated encephalopathy (SAE) is a common complication of sepsis, characterized by cognitive impairment, altered consciousness, and psychiatric symptoms, including anxiety and depression. These psychiatric symptoms often exacerbate the overall prognosis and quality of life of affected patients. However, the underlying metabolic and proteomic features associated with SAE-induced psychiatric symptoms remain poorly understood.
Aim: To investigate the clinical manifestations of anxiety and depression in patients with sepsis and SAE and to explore their associated metabolic and proteomic characteristics.
Methods: A total of 88 patients were enrolled, comprising 30 healthy controls, 29 patients with sepsis, and 29 with SAE. Anxiety and depression symptoms were evaluated using the Hamilton anxiety rating scale (HAM-A) and Hamilton depression rating scale (HAM-D) in sepsis and SAE. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), and quality of life was measured using the 36-Item Short Form Health Survey. Plasma samples were analyzed for metabolomic and proteomic profiling. Metabolic alterations were identified through liquid chromatography-mass spectrometry, while protein expression was assessed using Olink targeted proteomics.
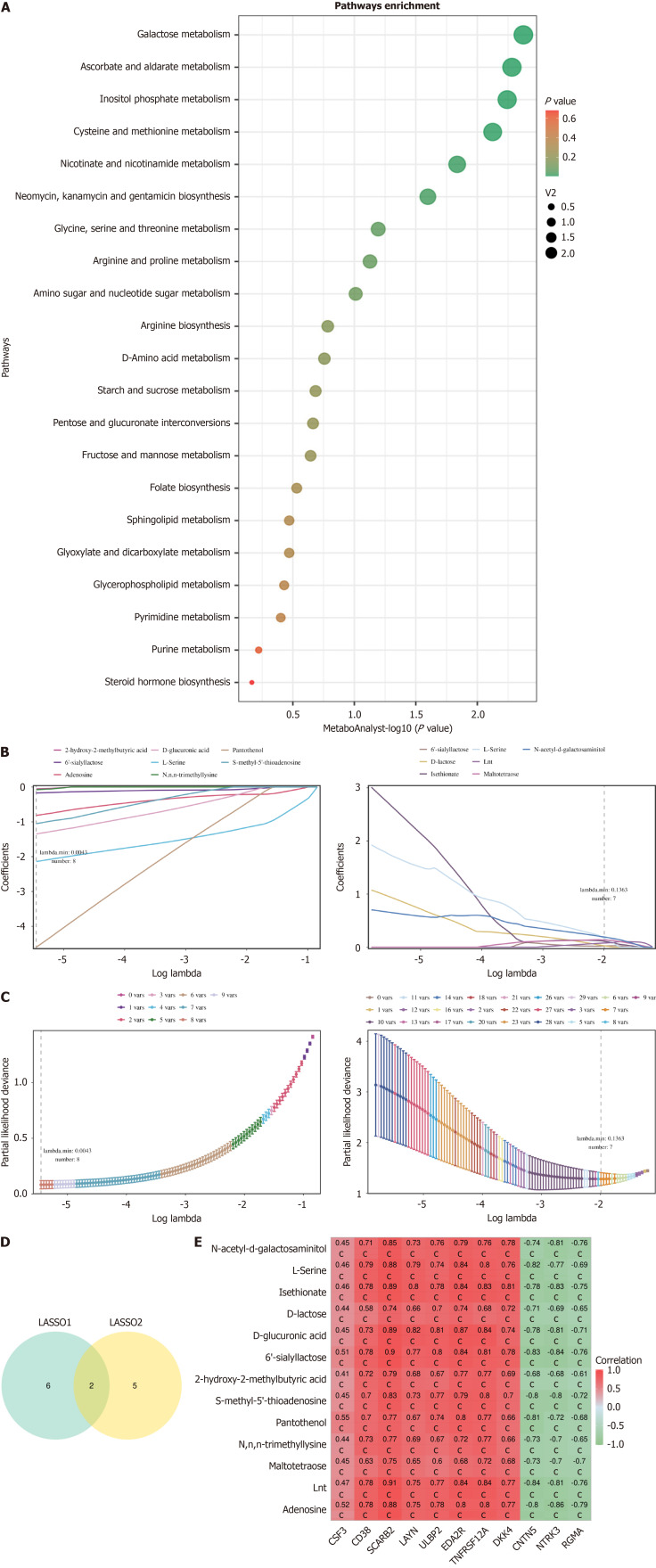
Results: Compared to the sepsis group, patients with SAE exhibited significantly higher levels of anxiety (HAM-A: 15.2 ± 4.0 vs 10.4 ± 3.0, P = 0.012) and depression (HAM-D: 16.0 ± 3.5 vs 9.1 ± 2.3, P = 0.003). Cognitive function, as measured by MoCA, was notably impaired in the SAE group (MoCA: 18.5 ± 4.0 vs 24.5 ± 3.2, P = 0.007). Quality of life scores, particularly in physical functioning, emotional well-being, and mental health, were significantly lower in patients with SAE. Metabolomic and proteomic analyses revealed substantial alterations in oxidative stress and nicotinamide adenine dinucleotide (NAD+) metabolism pathways, with cluster of differentiation (CD) 38 emerging as a potential biomarker associated with psychiatric symptoms in SAE. Further validation in an independent cohort confirmed the diagnostic relevance of CD38.
Conclusion: This study highlights the significant psychological burden of SAE, manifested as anxiety and depression. Multi-omics analysis identified distinct metabolic alterations, particularly in NAD+ metabolism, that may contribute to psychiatric symptom development and progression. Furthermore, CD38 was identified as a promising biomarker for the early detection of SAE, providing potential avenues for early intervention and therapeutic targeting.
Keywords: Anxiety; Cluster of differentiation 38; Depression; Metabolomics; Proteomics; Sepsis-associated encephalopathy.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures





References
LinkOut - more resources
Full Text Sources
Research Materials
