

Exercise capacity in heart failure: a systematic review and meta-analysis of HFrEF and HFpEF disparities in VO2peak and 6-minute walking distance
- PMID: 40574807
- PMCID: PMC12202100
- DOI: 10.1093/ehjopen/oeaf055
Exercise capacity in heart failure: a systematic review and meta-analysis of HFrEF and HFpEF disparities in VO2peak and 6-minute walking distance
Abstract
Aims: Heart failure (HF) with reduced ejection fraction (HFrEF) and HF with preserved ejection fraction (HFpEF) exhibit unique physiological pathways, influencing exercise capacity and functional performance. This systematic review and meta-analysis aimed to compare peak oxygen consumption (VO2peak), six-minute walk distance (6MWD), cardiac output (CO), and stroke volume (SV), between these phenotypes.
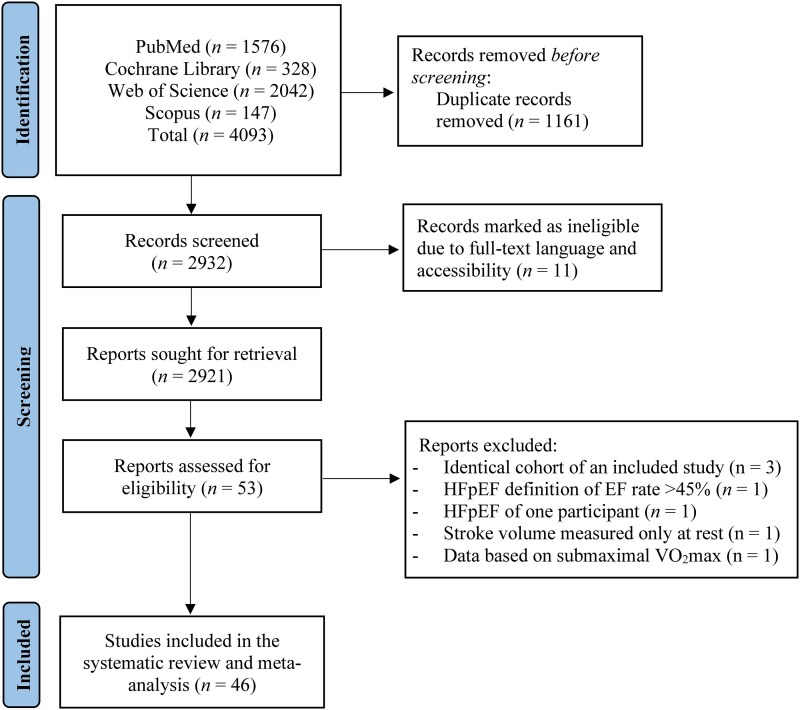
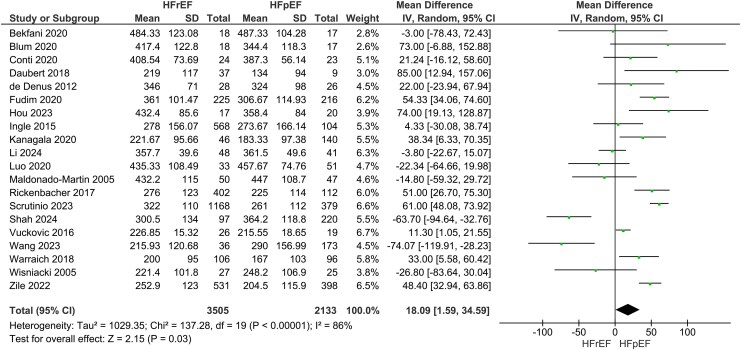
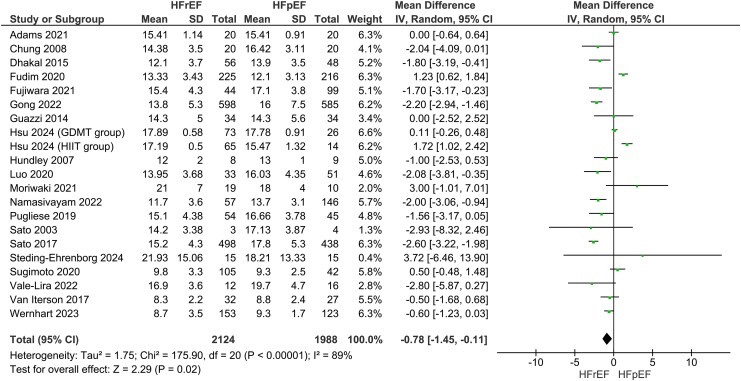
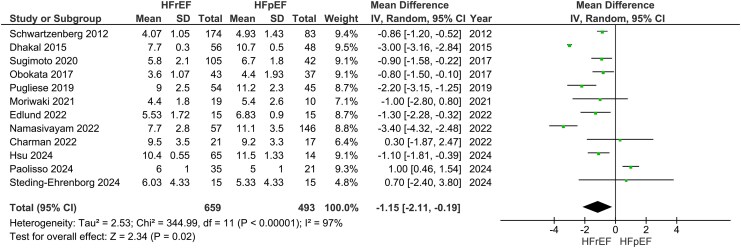
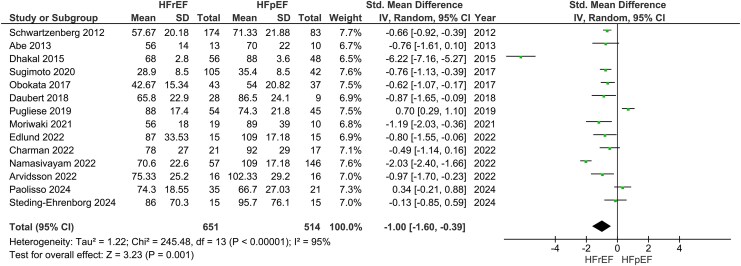
Methods and results: A systematic literature search of cohort studies via databases (PubMed, Web of Science, Scopus, and Cochrane Library) was conducted from inception until October 2024. A meta-analysis using a random-effects model to calculate the pooled effects was employed. Forty-six studies were included. HFrEF patients demonstrated significantly greater 6MWD compared to HFpEF (k = 20; mean difference (MD): 18.09 m, 95% confidence interval (CI) 1.59-34.59, I2 = 86%, P = 0.03), though this difference became insignificant after adjusting for comorbidities. Conversely, HFpEF patients exhibited higher VO2peak (k = 20; MD: -0.78 mL/kg/min, 95% CI -1.45--0.11, I2 = 89%, P = 0.02), CO (k = 12; MD: -1.15 L/min, 95% CI -2.11--0.19, I2 = 97%, P = 0.02), and SV (k = 14; SMD: -1.00, 95% CI -1.60--0.39, I2 = 95%, P < 0.01). Age was identified as a significant moderator of VO2peak.
Conclusion: HFpEF patients demonstrated superior VO2peak, CO, and SV compared to HFrEF patients, while the observed 6MWD advantage in HFrEF was likely influenced by comorbidities. Our findings emphasize the importance of tailoring rehabilitation strategies to HF phenotype-specific physiological profiles, particularly focusing on improving VO2peak and cardiac efficiency in HFpEF.
Keywords: HFpEF; HFrEF; Heart failure; Physical function; VO2peak.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Similar articles
-
Pulmonary rehabilitation versus usual care for adults with asthma.Cochrane Database Syst Rev. 2022 Aug 22;8(8):CD013485. doi: 10.1002/14651858.CD013485.pub2. Cochrane Database Syst Rev. 2022. PMID: 35993916 Free PMC article.
-
The Effectiveness of Lifestyle Interventions in Heart Failure With Preserved Ejection Fraction: A Systematic Review and Network Meta-Analysis.J Card Fail. 2024 Aug;30(8):994-1009. doi: 10.1016/j.cardfail.2024.01.015. Epub 2024 Feb 29. J Card Fail. 2024. PMID: 38428727
-
Exercise training in heart failure patients with preserved ejection fraction: a systematic review and meta-analysis.Monaldi Arch Chest Dis. 2016 Oct 14;86(1-2):759. doi: 10.4081/monaldi.2016.759. Monaldi Arch Chest Dis. 2016. PMID: 27748473
-
Neuromuscular electrostimulation for adults with chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2018 May 29;5(5):CD010821. doi: 10.1002/14651858.CD010821.pub2. Cochrane Database Syst Rev. 2018. PMID: 29845600 Free PMC article.
-
Sodium-glucose co-transporter 2 inhibitors in heart failure with mildly reduced or preserved ejection fraction: an updated systematic review and meta-analysis.Eur J Med Res. 2022 Dec 29;27(1):314. doi: 10.1186/s40001-022-00945-z. Eur J Med Res. 2022. PMID: 36581880 Free PMC article.
References
-
- Braunwald E. Cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med 1997;337:1360–1369. - PubMed
-
- McDonagh TA, Metra M, Adamo M, , Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Piepoli MF, Price S, Rosano GMC, Ruschitzka F, Skibelund AK; ESC Scientific Document Group . 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Rev Esp Cardiol (Engl Ed). 2022;75:523. - PubMed
-
- Del Buono MG, Arena R, Borlaug BA, Carbone S, Canada JM, Kirkman DL, Garten R, Rodriguez-Miguelez P, Guazzi M, Lavie CJ, Abbate A. Exercise intolerance in patients with heart failure: JACC state-of-the-art review. J Am Coll Cardiol 2019;73:2209–2225. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
