

Impact of cardiac rehabilitation and treatment compliance after ST-segment elevation myocardial infarction (STEMI) in France, the STOP SCA+ study
- PMID: 40574816
- PMCID: PMC12198249
- DOI: 10.3389/fcvm.2025.1484401
Impact of cardiac rehabilitation and treatment compliance after ST-segment elevation myocardial infarction (STEMI) in France, the STOP SCA+ study
Erratum in
-
Correction: Impact of cardiac rehabilitation and treatment compliance after ST-segment elevation myocardial infarction (STEMI) in France, the STOP SCA+ study.Front Cardiovasc Med. 2025 Sep 11;12:1656799. doi: 10.3389/fcvm.2025.1656799. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 41019441 Free PMC article.
Abstract
Introduction: Acute ST-elevation myocardial infarction (STEMI) is a frequent and serious presentation of acute coronary syndrome. The STOP-SCA+ study aimed to (i) describe 1-year compliance to secondary prevention cardiac tri-therapy and (ii) identify factors associated with negative outcomes 1 year after STEMI, particularly the impact of compliance and rehabilitation care.
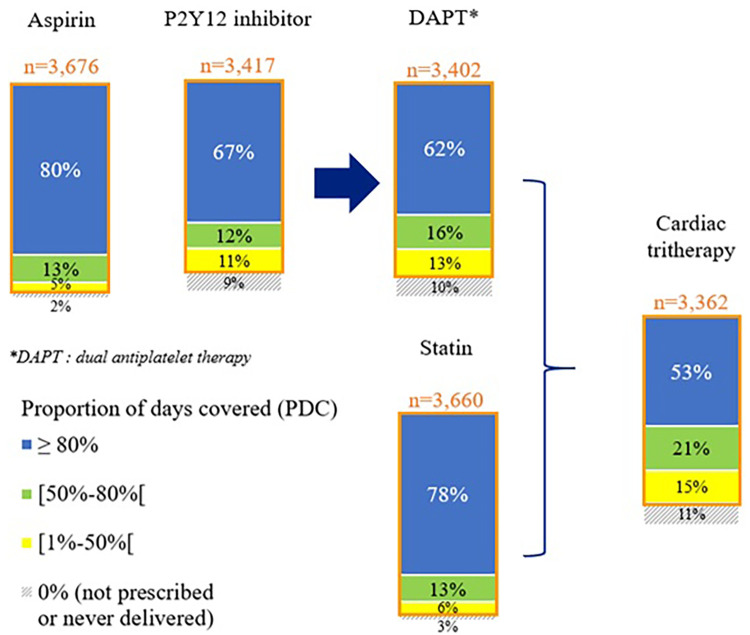
Methods: Patients who were >18 years old and hospitalized for STEMI in five interventional cardiac centers with the same cardiac registry in one French region (2.5 million inhabitants), between 2014 and 2018, were included. After a probabilistic matching with the National Health Insurance database [Système National des Données de Santé (SNDS), 96% matching], compliance for cardiac tri-therapy was studied: aspirin, P2Y12 inhibitor, and statin. Factors associated with poor outcomes (ischemic complications, death) were analyzed using Cox modeling and those for compliance by logistic regression.
Results: A total of 3,768 patients were included, of whom 84% underwent primary percutaneous coronary intervention. At 1 year, 3,362 had at least one tri-therapy delivery (89.2%), of whom 53% were compliant, and 2,478 patients went to cardiac rehabilitation (65.8%). Death occurred in 130 patients and/or ischemic complications in 194 (total of poor outcomes 8.0%). Compliance was not associated with complications over the year [HR 1.16 (0.86-1.57)], while the absence of cardiac rehabilitation [2.31 (1.73-3.08)] was associated, as well as female sex 1.54 (1.08-2.19), renal impairment [2.87 (1.49-5.53)], initial STEMI clinical presentation [pejorative Killip 2.04 (1.19-3.50)], and LVEF <40% at discharge [2.22 (1.65-2.99)]. Additionally, cardiac rehabilitation was associated with compliance [OR 1.55 (1.34-1.79)].
Discussion: Pejorative outcomes 1 year after a STEMI represented 8% of cases, mainly related to patient features, the initial clinical presentation, and the absence of access to rehabilitation. Compliance part in patient health outcomes will need further modeling to accurately study its impact. Matching clinical and medico-administrative databases proved to be relevant for assessing outcomes at a large scale.
Keywords: cardiac rehabilitation; compliance; myocardial infarction (MI); outcome; probabilistic matching.
© 2025 Laurent, Godillon, Tassi, Marcollet, Chassaing, Decomis, Bezin, Laure, Angoulvant, Range and Grammatico-Guillon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer EG declared a shared affiliation with the author JB to the handling editor at the time of review.
Figures


References
-
- Direction de la recherche, des études, de l’évaluation et des statistiques/Santé publique France. L’état de santé de la population en France Rapport 2017—Principales causes de décès et de mortalité. (2017). Available at: https://drees.solidarites-sante.gouv.fr/sites/default/files/2021-01/Prin... (Accessed 3 October, 2023).
-
- Santé Publique France. Infarctus du myocarde. Available at: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-car... (Accessed 12 April, 2023).
-
- Rangé G, Chassaing S, Marcollet P, Saint-Étienne C, Dequenne P, Goralski M, et al. The CRAC cohort model: a computerized low cost registry of interventional cardiology with daily update and long-term follow-up. Rev Epidemiol Sante Publique. (2018) 66:209–16. 10.1016/j.respe.2018.01.135 - DOI - PubMed
-
- Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European society of cardiology (ESC). Eur Heart J. (2023) 44:3720–3826. 10.1093/eurheartj/ehad191 - DOI - PubMed
LinkOut - more resources
Full Text Sources