

Cost-effectiveness of FIT and a FIT-based model to optimise symptomatic diagnosis of colorectal cancer: health economic modelling for the COLOFIT project
- PMID: 40575070
- PMCID: PMC12198831
- DOI: 10.1136/bmjph-2024-002089
Cost-effectiveness of FIT and a FIT-based model to optimise symptomatic diagnosis of colorectal cancer: health economic modelling for the COLOFIT project
Abstract
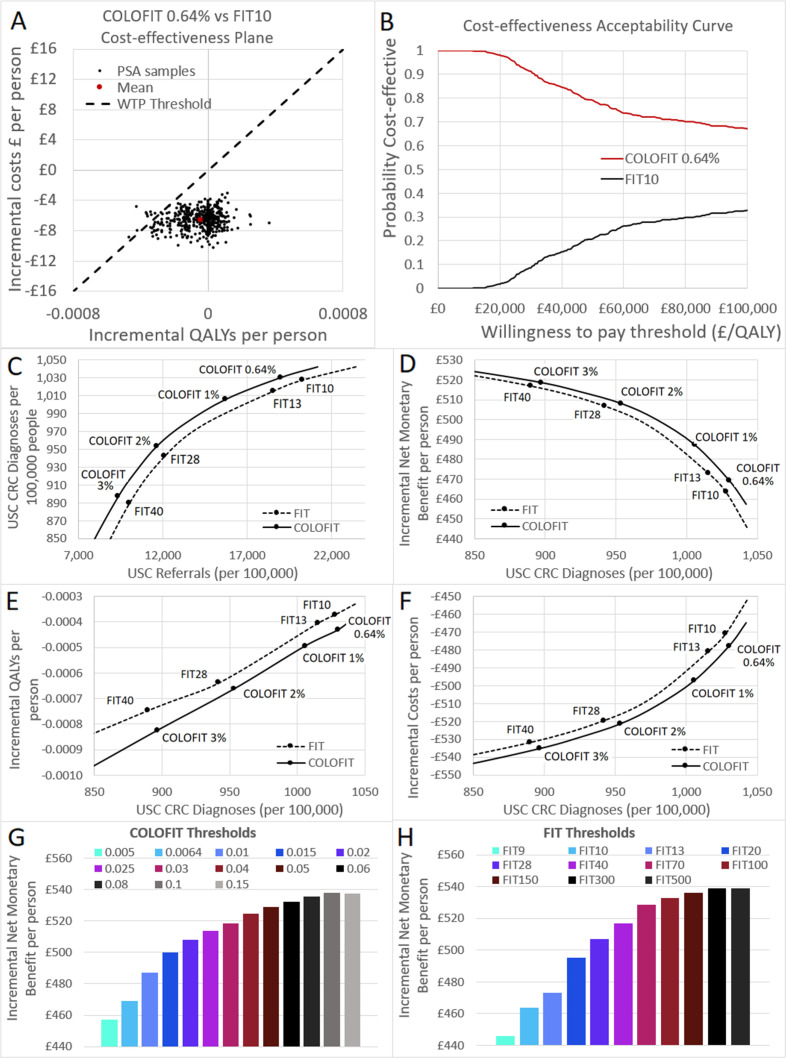
Introduction: Fecal immunochemical testing (FIT) at a threshold of 10 mg haemaglobin (Hb)/g is used in English primary care to prioritise urgent referral for colorectal cancer (CRC) investigation in symptomatic patients. The COLOFIT algorithm, based on FIT score, age, sex and blood results, performs better than FIT alone for identifying CRC. We assessed the cost-effectiveness of COLOFIT compared with FIT and investigated optimal risk thresholds.
Methods: An individual patient-level simulation model was developed, with synthetic populations constructed from data used to validate COLOFIT. Referral criteria based on different FIT scores and COLOFIT-assessed risk thresholds were modelled using probabilistic and scenario analyses. Outcomes included costs, quality-adjusted life years (QALYs) and cost-effectiveness measured using incremental net monetary benefit (INMB) based on a willingness to pay threshold of £20 000/QALY.
Results: COLOFIT at a CRC risk threshold of 0.64% has a 98% probability of being more cost-effective than FIT 10 mg Hb/g (INMB is £5.67 per person), while detecting similar numbers of cancers. Cost-effectiveness is achieved by cost savings from reducing referrals outweighing QALYs lost through reorienting expedited CRC diagnoses from younger (<50) to older (≥70) patients. Cost-effectiveness improves as risk thresholds rise. High structural uncertainty around cancer progression during diagnostic delay and diagnosis of other serious bowel diseases considerably affects cost-effectiveness.
Conclusions: COLOFIT is likely to be more cost-effective than FIT alone and could help alleviate pressure on diagnostic services. However, strategies to improve diagnosis in the under 50s would be necessary to mitigate potential harm. Further research should assess how COLOFIT impacts cancer survival and diagnosis of other serious bowel diseases.
Keywords: Risk Assessment; economics; statistics and numerical data.
Copyright © Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
None declared.
Figures


References
-
- Bowel cancer statistics: cancer research UK. 2022. https://www.cancerresearchuk.org/health-professional/cancer-statistics/s... Available.
-
- Early diagnosis data hub: cancer research UK cancer intelligence team. 2022. https://crukcancerintelligence.shinyapps.io/EarlyDiagnosis/ Available.
-
- NICE NG12 suspected cancer: recognition and referral. 2023. https://www.nice.org.uk/guidance/ng12 Available. - PubMed
LinkOut - more resources
Full Text Sources