

Comparison of treatment strategies for submucosal tumors originating from the muscularis propria at esophagogastric junction or cardia
- PMID: 40575341
- PMCID: PMC12188769
- DOI: 10.3748/wjg.v31.i23.106261
Comparison of treatment strategies for submucosal tumors originating from the muscularis propria at esophagogastric junction or cardia
Abstract
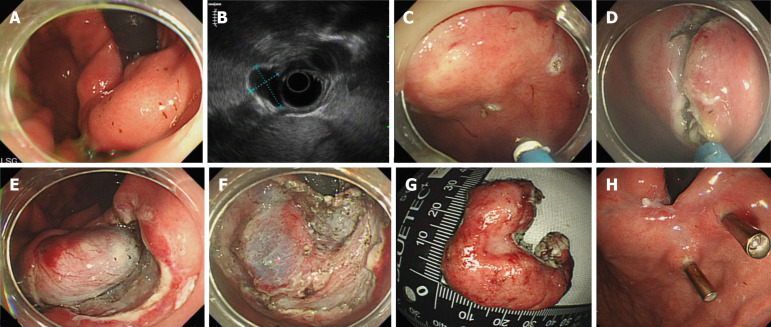
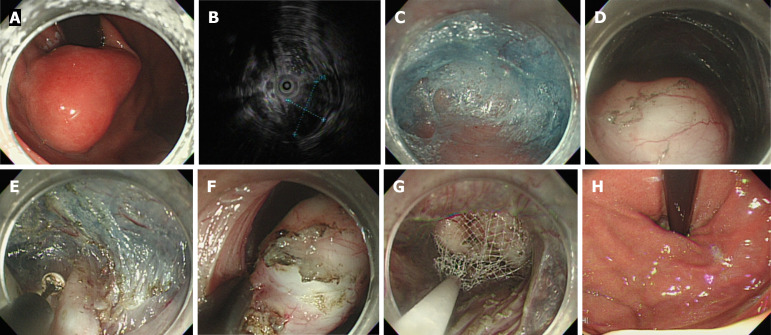
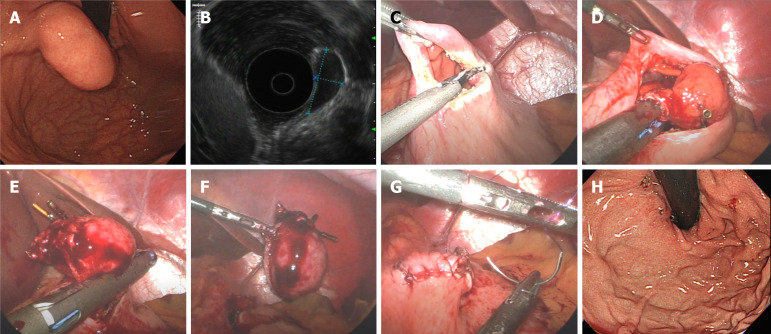
Background: The spectrum of gastric submucosal tumors (SMTs) in the upper gastrointestinal system ranges from non-neoplastic to malignant lesions, with gastrointestinal stromal tumors exhibiting inherent malignant potential. However, the diagnosis of SMTs remains challenging, and treatment methods, especially for tumors located at the cardia or esophagogastric junction (EGJ), are not well established. Minimally invasive techniques - such as endoscopic submucosal dissection (ESD), submucosal tunneling endoscopic resection (STER), and laparoscopic wedge resection (LWR) - have been developed for these lesions. However, comparative data on their feasibility, safety, and clinical outcomes in these locations remain limited.
Aim: To compare ESD, STER, and LWR for SMTs at the EGJ or cardia, focusing on procedural feasibility.
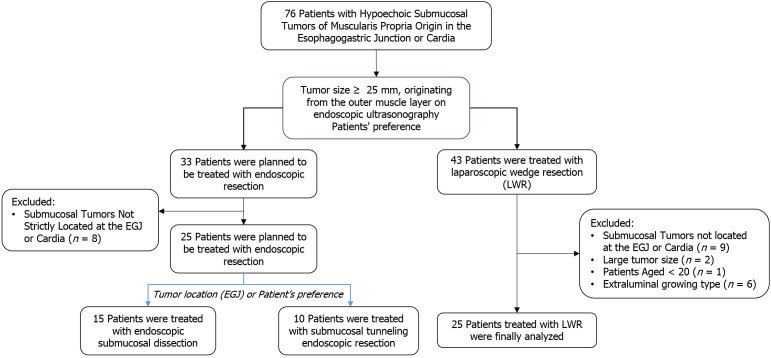
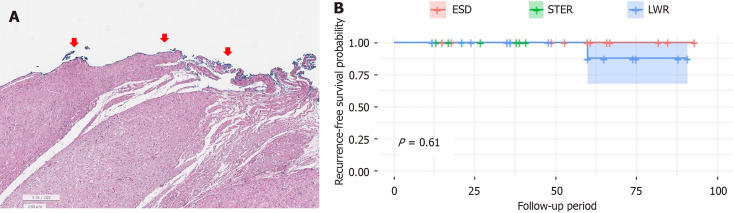
Methods: This single-center retrospective study included patients with SMTs less than 45 mm from the muscularis propria, growing intraluminally at the EGJ or cardia, and treated with ESD, STER, or LWR between July 2014 and September 2022. The primary outcome was relapse-free survival during follow-up.
Results: The median age (interquartile range) was 53.0 (40.0-57.5), 43.0 (39.0-57.0), and 56.0 (43.0-64.0) years for ESD, STER, and LWR, respectively. The median follow-up time (interquartile range) was 60.0 (26.5-66.5), 24.0 (13.0-38.0), and 35.0 (21.0-60.0) months. LWR had the largest tumors (30.0 mm) and the highest rate of high-risk gastrointestinal stromal tumors (68.0%, P < 0.001). Tumor recurrence occurred in one LWR patient (4.0%, P = 0.600). En bloc and macroscopic resection rates were 100% (P = 1.000), but microscopic resection rates differed (P = 0.021). Significant minor complications occurred in 5 patients (10.0%), all grade IIIa. Tumor location (cardia/fundus, P = 0.006) and prolonged procedure time (P < 0.001) were significantly associated with complications.
Conclusion: ESD, STER, and LWR are effective for SMTs at the EGJ and cardia, with minor complications associated with tumor location and procedure time, and comparable recurrence rates.
Keywords: Cardia; Esophagogastric junction; Gastrointestinal stromal tumors; Minimally invasive surgical procedures; Muscularis propria.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
Similar articles
-
Submucosal tunneling endoscopic resection: An effective and safe therapy for upper gastrointestinal submucosal tumors originating from the muscularis propria layer.World J Gastroenterol. 2019 Jan 14;25(2):245-257. doi: 10.3748/wjg.v25.i2.245. World J Gastroenterol. 2019. PMID: 30670913 Free PMC article.
-
Submucosal tumors of the esophagogastric junction originating from the muscularis propria layer: a large study of endoscopic submucosal dissection (with video).Gastrointest Endosc. 2012 Jun;75(6):1153-8. doi: 10.1016/j.gie.2012.01.037. Epub 2012 Mar 28. Gastrointest Endosc. 2012. PMID: 22459663 Clinical Trial.
-
Submucosal tunneling endoscopic resection of large submucosal tumors originating from the muscularis propria layer in the esophagus and gastric cardia.Z Gastroenterol. 2019 Aug;57(8):952-959. doi: 10.1055/a-0905-3173. Epub 2019 Aug 9. Z Gastroenterol. 2019. PMID: 31398766 English.
-
Endoscopic resection of esophageal and gastric submucosal tumors from the muscularis propria layer: submucosal tunneling endoscopic resection versus endoscopic submucosal excavation: A systematic review and meta-analysis.Surg Endosc. 2021 Dec;35(12):6413-6426. doi: 10.1007/s00464-021-08659-9. Epub 2021 Aug 20. Surg Endosc. 2021. PMID: 34415431
-
The Impact of Traction Methods on Endoscopic Submucosal Dissection Efficacy for Gastric Neoplasia: A Systematic Review and Meta-analysis.J Gastrointest Cancer. 2024 Mar;55(1):129-142. doi: 10.1007/s12029-023-00982-9. Epub 2023 Nov 13. J Gastrointest Cancer. 2024. PMID: 37953438
References
-
- Chak A. EUS in submucosal tumors. Gastrointest Endosc. 2002;56:S43–S48. - PubMed
-
- Miettinen M, Lasota J. Gastrointestinal stromal tumors--definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch. 2001;438:1–12. - PubMed
-
- Polkowski M. Endoscopic ultrasound and endoscopic ultrasound-guided fine-needle biopsy for the diagnosis of malignant submucosal tumors. Endoscopy. 2005;37:635–645. - PubMed
-
- Rösch T, Kapfer B, Will U, Baronius W, Strobel M, Lorenz R, Ulm K German EUS Club. Endoscopic ultrasonography. Accuracy of endoscopic ultrasonography in upper gastrointestinal submucosal lesions: a prospective multicenter study. Scand J Gastroenterol. 2002;37:856–862. - PubMed
-
- Gress F, Schmitt C, Savides T, Faigel DO, Catalano M, Wassef W, Roubein L, Nickl N, Ciaccia D, Bhutani M, Hoffman B, Affronti J. Interobserver agreement for EUS in the evaluation and diagnosis of submucosal masses. Gastrointest Endosc. 2001;53:71–76. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
