

Embolization of a high cervical pial arteriovenous fistula resulting in respiratory insufficiency due to diaphragmatic paralysis: A case report
- PMID: 40575369
- PMCID: PMC12197895
- DOI: 10.1016/j.radcr.2025.05.060
Embolization of a high cervical pial arteriovenous fistula resulting in respiratory insufficiency due to diaphragmatic paralysis: A case report
Abstract
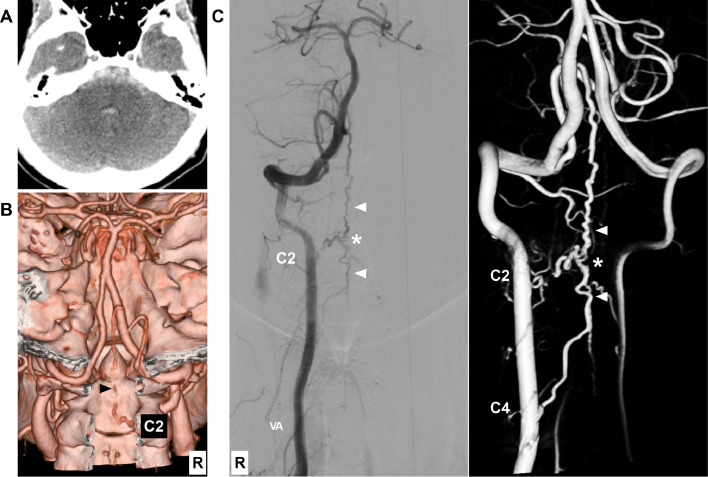
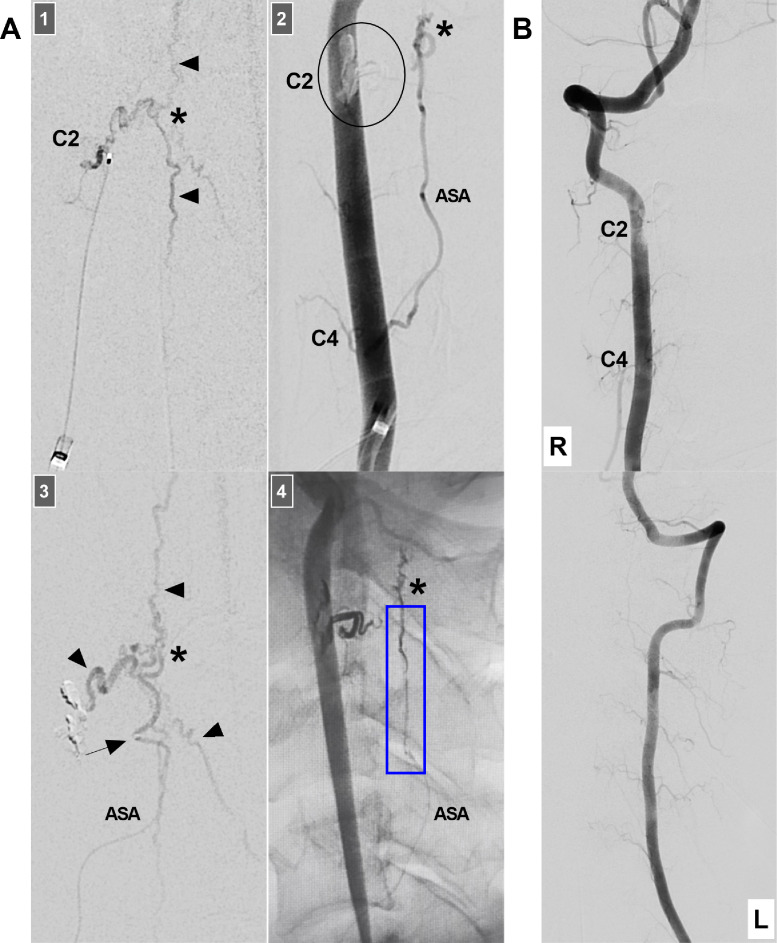
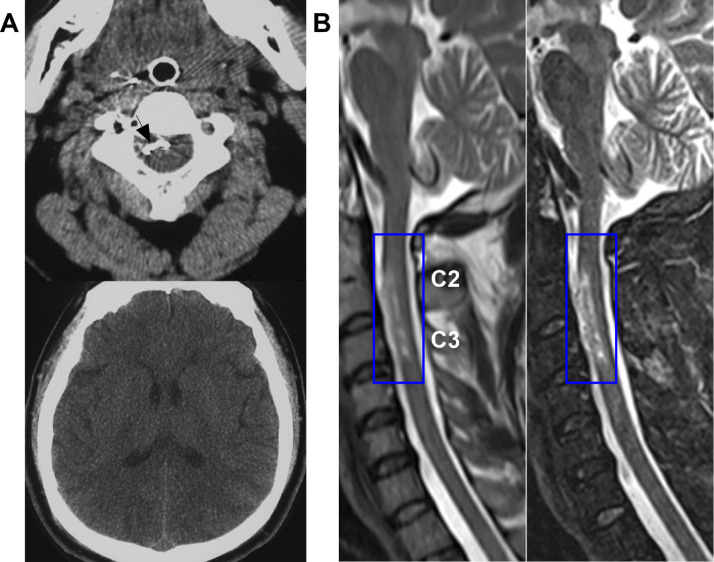
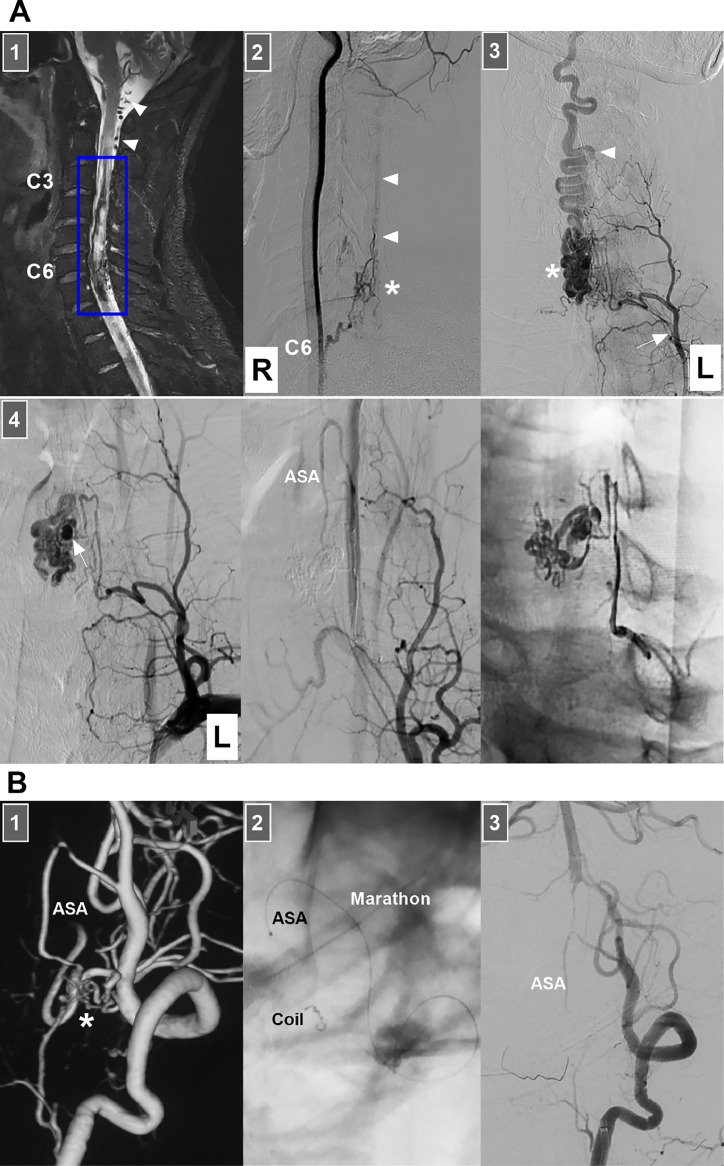
When endovascular treatment (EVT) is administered via the anterior spinal artery (ASA) for high cervical pial arteriovenous fistulas (PAVFs), severe diaphragmatic paralysis, although rare, may occur. We report a 46-year-old male who experienced subarachnoid hemorrhage. The Hunt-Hess scale score was Grade II. Angiography revealed a high cervical PAVF supplied by the C2 radiculomedullary artery and the ASA at the C4 vertebra level. EVT was performed. A microcatheter introduced through the ASA was placed close to the PAVF. After the Onyx agent was cast, the PAVF was obliterated; however, Onyx reflux into the ASA trunk was observed. Postoperatively, the patient had hemiparesis and insufficient autonomous respiration and mechanical ventilation was provided. Fifteen days after EVT, the patient's hemiparesis completely resolved. Ultrasound examination revealed diaphragmatic paralysis. Magnetic resonance imaging revealed cervical cord infarction at the C2-C3 vertebral level, which supported the diagnosis of diaphragmatic paralysis due to phrenic nerve injury from cervical cord infarction above the C4 level. Respiratory function training was performed daily. Eighty-seven days after EVT, his autonomous respiration function further improved. However, 93 days after EVT, the patient died while asleep because the portable ventilator was not used. Therefore, for EVT for high cervical PAVFs, excessive Onyx reflux into the ASA can result in ventral cervical cord infarction, causing severe respiratory insufficiency due to diaphragmatic paralysis. We reported this case to alert neurointerventionists to the lessons learned from experience.
Keywords: Anterior spinal artery; Cervical cord; Diaphragmatic paralysis; Embolization; Pial arteriovenous fistula.
© 2025 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
References
-
- Meng X., Zhang H., Wang Y., Ye M., He C., Du J., et al. Perimedullary arteriovenous fistulas in pediatric patients: clinical, angiographical, and therapeutic experiences in a series of 19 cases. Childs Nerv Syst. 2010;26(7):889–896. - PubMed
-
- Sasamori T., Hida K., Yano S., Asano T., Iwasaki Y. Cervical perimedullary arteriovenous fistula in an infant presenting with subarachnoid hemorrhage–case report. Neurol Med Chir (Tokyo) 2008;48(9):409–413. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
