

Extracorporeal cardiopulmonary resuscitation for pediatric in-hospital cardiac arrest in single ventricle patients: a systematic review and meta-analysis
- PMID: 40575376
- PMCID: PMC12192686
- DOI: 10.1016/j.resplu.2025.100997
Extracorporeal cardiopulmonary resuscitation for pediatric in-hospital cardiac arrest in single ventricle patients: a systematic review and meta-analysis
Abstract
Objectives: Assess the use of extracorporeal cardiopulmonary resuscitation (ECPR), compared with manual/mechanical cardiopulmonary resuscitation (CPR), for in-hospital cardiac arrest (IHCA) in pediatric patients with single ventricle (SV) congenital heart disease (CHD).
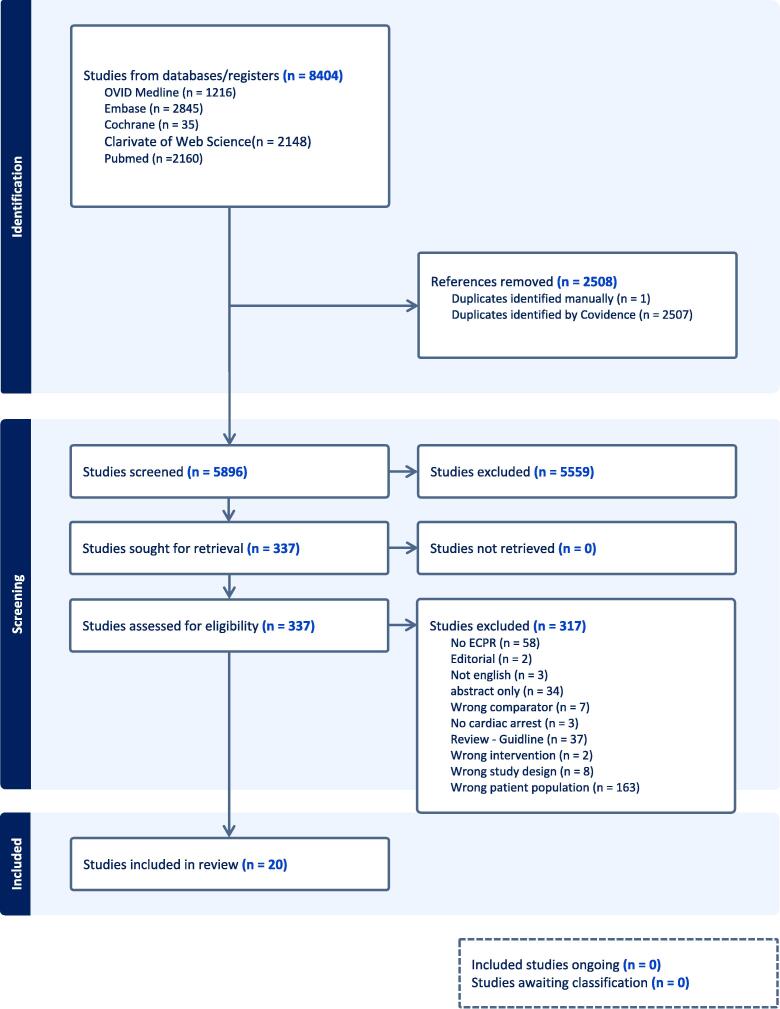
Methods: PRISMA guidelines were followed with PROSPERO registration (CRD42023479671). We searched Medline, Embase, Web of Science, PubMed, and the Cochrane Library for studies published before January 23, 2025. The population included pediatric patients (<18 years old) with IHCA. Two investigators reviewed studies for relevance, extracted data, and assessed risk of bias using the ROBINS-I tool. Certainty of evidence was evaluated using the GRADE framework. Outcomes included short-term and long-term survival and favorable neurological outcome.
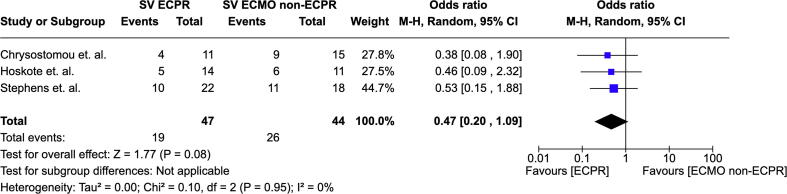
Results: We identified 20 studies: 15 described ECPR in SV patients without a comparator group, and 5 compared SV ECPR patients vs. SV extracorporeal membrane oxygenation (ECMO) without ECPR (ECMO non-ECPR). Pooled synthesis for survival to hospital discharge was analyzed in 3 observational studies with 91 SV patients (pooled OR 0.66, 95% CI 0.37-1.01) and separately in 2 registry studies with 968 SV patients (OR 0.76, 95% CI 0.35-1.37 and OR 1.06, 95% CI 0.78-1.41) with very low certainty of evidence (downgraded for risk of bias and imprecision). These studies found no significant difference in survival to hospital discharge in ECPR compared to ECMO non-ECPR in pediatric SV patients. No studies were identified that compared pediatric SV patients who received ECPR vs. conventional/manual CPR.
Conclusions: There is no direct evidence to either support or refute the use of ECPR during IHCA in pediatric patients with SV CHD, and there is inconclusive evidence to either support or refute the use of ECPR compared to ECMO non-ECPR. Additional research is needed to address the use of ECPR in this specific cardiac population.
Keywords: Cardiac arrest; Children; ECPR; Extracorporeal cardiopulmonary resuscitation; Single ventricle.
© 2025 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: “This work was conducted through volunteer support from the International Liaison Committee On Resuscitation (ILCOR) who receives funding from the American Heart Association. The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Collaborator MK, KCN, and AT are Editorial Board members of Resuscitation Plus”.
Figures
Similar articles
-
Continuous chest compression versus interrupted chest compression for cardiopulmonary resuscitation of non-asphyxial out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2017 Mar 27;3(3):CD010134. doi: 10.1002/14651858.CD010134.pub2. Cochrane Database Syst Rev. 2017. PMID: 28349529 Free PMC article.
-
Extracorporeal cardiopulmonary resuscitation for cardiac arrest: An updated systematic review.Resuscitation. 2023 Jan;182:109665. doi: 10.1016/j.resuscitation.2022.12.003. Epub 2022 Dec 12. Resuscitation. 2023. PMID: 36521684
-
Extracorporeal-CPR Versus Conventional-CPR for Adult Patients in Out of Hospital Cardiac Arrest- Systematic Review and Meta-Analysis.J Intensive Care Med. 2025 Feb;40(2):207-217. doi: 10.1177/08850666241303851. Epub 2024 Dec 5. J Intensive Care Med. 2025. PMID: 39635840
-
Prognostic effects of cardiopulmonary resuscitation (CPR) start time and the interval between CPR to extracorporeal cardiopulmonary resuscitation (ECPR) on patient outcomes under extracorporeal membrane oxygenation (ECMO): a single-center, retrospective observational study.BMC Emerg Med. 2024 Mar 5;24(1):36. doi: 10.1186/s12873-023-00905-8. BMC Emerg Med. 2024. PMID: 38438853 Free PMC article.
-
Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients.Cochrane Database Syst Rev. 2021 Jul 19;7(7):CD013307. doi: 10.1002/14651858.CD013307.pub2. Cochrane Database Syst Rev. 2021. PMID: 34280303 Free PMC article.
References
-
- Conrad S.A., Broman L.M., Taccone F.S., et al. The extracorporeal life support organization Maastricht treaty for nomenclature in extracorporeal life support. A position paper of the Extracorporeal life support organization. Am J Respir Crit Care Med. 2018;198:447–451. doi: 10.1164/rccm.201710-2130CP. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
