

TENT5A-associated osteogenesis imperfecta: long-term follow-up and molecular insights
- PMID: 40575455
- PMCID: PMC12202044
- DOI: 10.1093/jbmrpl/ziaf083
TENT5A-associated osteogenesis imperfecta: long-term follow-up and molecular insights
Abstract
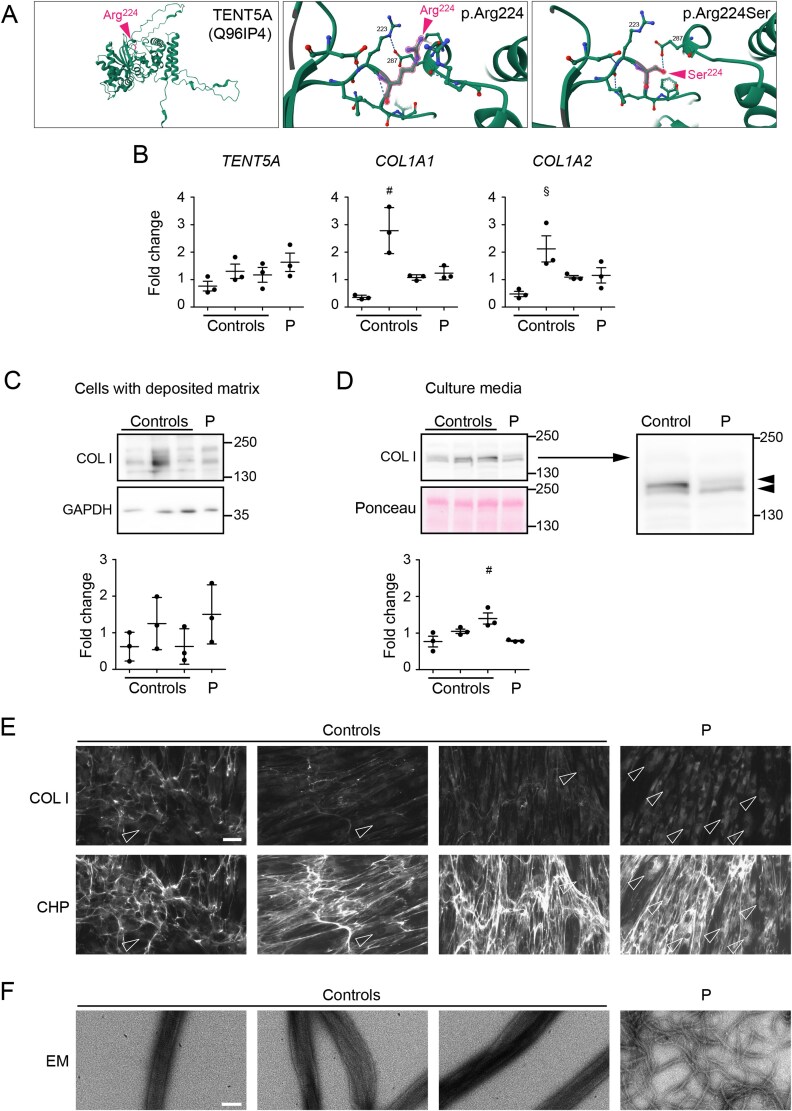
OI is a genetically diverse disorder characterized by bone fragility and deformities, with most cases attributed to dominant mutations in collagen I-related genes. However, mutations in TENT5A, encoding a poly(A) polymerase, have recently been implicated in severe, recessive forms of OI. We reported 3 individuals from a consanguineous family with a novel homozygous TENT5A variant (c.672G>T, p.Arg224Ser). Our patients presented with severe bone fragility, generalized osteopenia, skeletal deformities, short stature, and early wheelchair dependence. Patient-derived fibroblasts demonstrated impaired collagen secretion and disorganized fibril network formation. Our findings provide new insights into the complex pathophysiology of TENT5A-associated OI and underscore the need for further research into its role in skeletal homeostasis.
Keywords: FAM46a; bisphosphonates; collagen I; growth hormone deficiency; skeletal dysplasias.
© The Author(s) 2025. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Bisphosphonate therapy for osteogenesis imperfecta.Cochrane Database Syst Rev. 2016 Oct 19;10(10):CD005088. doi: 10.1002/14651858.CD005088.pub4. Cochrane Database Syst Rev. 2016. PMID: 27760454 Free PMC article.
-
Case Report: Holistic approach to management of an infant with severe osteogenesis imperfecta in the neonatal intensive care unit.Front Pediatr. 2025 Jun 11;13:1475545. doi: 10.3389/fped.2025.1475545. eCollection 2025. Front Pediatr. 2025. PMID: 40567522 Free PMC article.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher's disease: a systematic review.Health Technol Assess. 2006 Jul;10(24):iii-iv, ix-136. doi: 10.3310/hta10240. Health Technol Assess. 2006. PMID: 16796930
-
Case Series of 6 Fetuses With Osteogenesis Imperfecta Type II: A Retrospective Study of Heart Pathology.Pediatr Dev Pathol. 2025 Jan-Feb;28(1):24-30. doi: 10.1177/10935266241272511. Epub 2024 Aug 27. Pediatr Dev Pathol. 2025. PMID: 39189102 Free PMC article.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.Health Technol Assess. 2008 Mar;12(3):iii-ix, xi-xiv, 1-208. doi: 10.3310/hta12030. Health Technol Assess. 2008. PMID: 18284894
References
LinkOut - more resources
Full Text Sources
