

Risk of COVID-19 infection among frontline healthcare workers during the COVID-19 pandemic
- PMID: 40575632
- PMCID: PMC12188883
- DOI: 10.5501/wjv.v14.i2.99663
Risk of COVID-19 infection among frontline healthcare workers during the COVID-19 pandemic
Abstract
Background: In the initial stages of the coronavirus disease 2019 (COVID-19) pandemic, healthcare workers (HCWs) who were immunologically naive to COVID-19, were exposed to a highly transmissible virus.
Aim: To compare infection risk among HCWs in high-risk (HR) and low-risk (LR) areas.
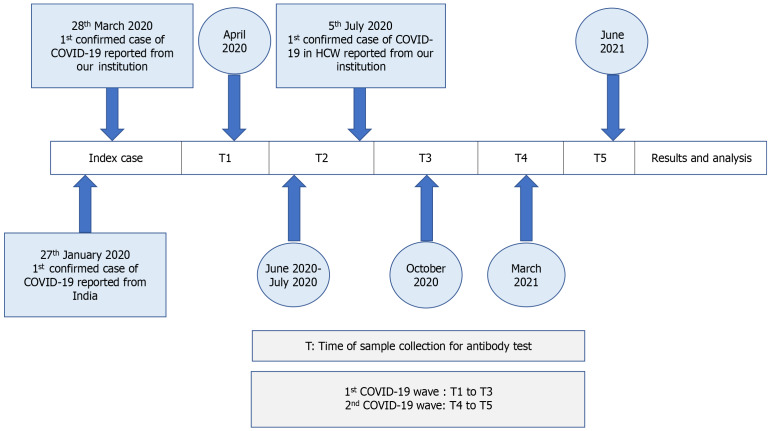
Methods: Data on reverse transcriptase-polymerase chain reaction confirmed clinical infection and samples for nucleocapsid, and spike protein antibodies were collected at five time-points (T1 to T5) from HCWs in the emergency department and intensive care unit (HR group) and pre-clinical and para-clinical areas (LR). For the sero-study, only participants who provided at least one baseline sample and one during the second wave (T4 or T5) were analysed. Since CovishieldTM elicits only spike protein antibodies, subclinical infection was diagnosed if asymptomatic unvaccinated and CovishieldTM vaccinated individuals tested positive for nucleocapsid antibody.
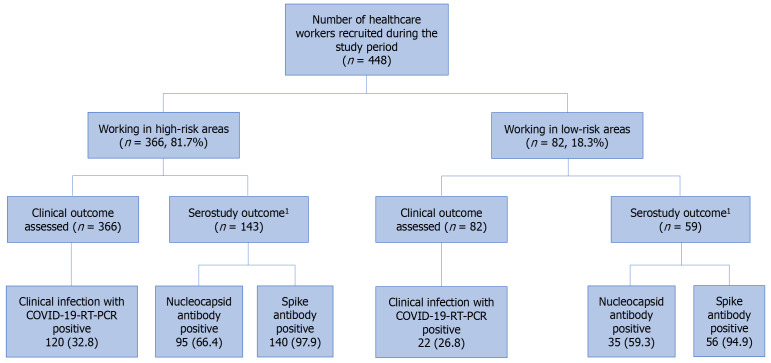
Results: Overall, by T5, clinical infection rate was similar in the HR (120/366, 32.8%) and LR (22/82, 26.8%) groups (P = 0.17). However, before vaccination (T3), more HCWs in the HR group developed COVID-19 infection (21.9% vs 8.8%, P = 0.046). In the sero-study group, clinical infection occurred in 31.5% (45/143) and 23.7% (14/59) in the HR and LR groups respectively (P = 0.23). Spike antibody was detected in 140/143 (97.9%) and 56/59 (94.9%) and nucleocapsid antibody was positive in 95/143 (66.4%) and 35/59 (59.3%) in the HR and LR groups respectively (P = 0.34). Subclinical infection rate (HR 34.9%, LR 35.6%, P = 0.37) and hospitalization rate were similar. There was no mortality.
Conclusion: Before vaccination, HCWs in HR areas had a higher risk of infection. Seroprevalence studies suggest that sub-clinical infection was not uncommon.
Keywords: COVID-19 pandemic; Healthcare workers; Nucleocapsid antibody; SARS-CoV-2 antibodies; Seroprevalence; Spike protein antibody.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
References
-
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int .
-
- Nguyen LH, Drew DA, Graham MS, Joshi AD, Guo CG, Ma W, Mehta RS, Warner ET, Sikavi DR, Lo CH, Kwon S, Song M, Mucci LA, Stampfer MJ, Willett WC, Eliassen AH, Hart JE, Chavarro JE, Rich-Edwards JW, Davies R, Capdevila J, Lee KA, Lochlainn MN, Varsavsky T, Sudre CH, Cardoso MJ, Wolf J, Spector TD, Ourselin S, Steves CJ, Chan AT COronavirus Pandemic Epidemiology Consortium. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. 2020;5:e475–e483. - PMC - PubMed
-
- Sim MR. The COVID-19 pandemic: major risks to healthcare and other workers on the front line. Occup Environ Med. 2020;77:281–282. - PubMed
-
- Los Angeles Times. Doctors and nurses fighting coronavirus in China die of both infection and fatigue. 2020. Available from: https://www.latimes.com/world-nation/story/2020-02-25/doctors-fighting-c... .
LinkOut - more resources
Full Text Sources
Miscellaneous
