

Impact of Socio-Economic, Behavioural and Clinical Factors on Liver Disease Progression in Individuals With HIV and Hepatitis B
- PMID: 40576003
- PMCID: PMC12203455
- DOI: 10.1111/liv.70191
Impact of Socio-Economic, Behavioural and Clinical Factors on Liver Disease Progression in Individuals With HIV and Hepatitis B
Abstract
Background and aims: Little is known about the contribution of sociodemographic and behavioural factors to developing liver disease in individuals with an HIV and chronic hepatitis B virus (HBV) co-infection. We aimed to quantify the impact of these factors on incident liver disease in individuals with HIV/HBV receiving care in the Netherlands.
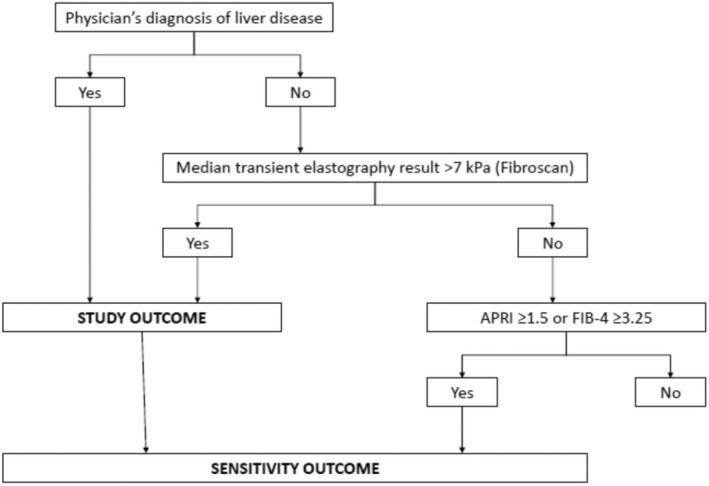
Methods: We used data from the Dutch observational ATHENA cohort combined with Statistics Netherlands. We included all hepatitis B surface antigen-positive individuals with HIV in care from 2008-2022. Severe liver disease (i.e., significant fibrosis (≥F2), cirrhosis, hepatocellular carcinoma, liver transplantation) was defined by physician diagnosis or a transient elastography result > 7 kPa. Determinants of incident liver disease were assessed using Cox proportional hazard models.
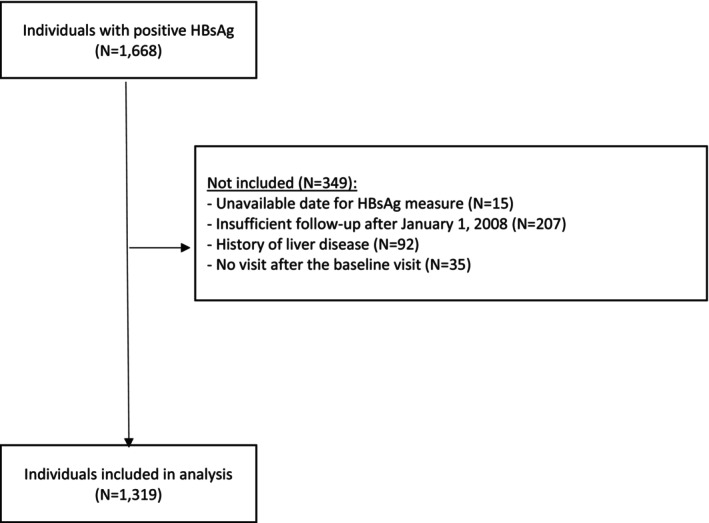
Results: In the 1319 individuals included (12,277 person-years (PY); 93.3% HIV-RNA < 200 copies/ml), the incidence rate of severe liver disease was 0.59 per 100 PY [95% confidence interval (CI) = 0.47-0.75]. After adjustment for age and time since HBV diagnosis, tobacco smoking, HCV coinfection and body mass index > 25 kg/m2 increased the risk of liver disease [adjusted hazards ratio (aHR) = 2.33, 95% CI = 1.38-3.94; aHR = 4.00, 95% CI = 2.18-7.33, aHR = 1.75, 95% CI = 1.05-2.92, respectively]. Conversely, men who have sex with men (vs. other transmission routes, aHR = 0.54, 95% CI = 0.32-0.90), and individuals living in an urbanised municipality (aHR = 0.50, 95% CI = 0.30-0.85) had a reduced risk of liver disease.
Conclusions: Liver disease progression in people living with HIV/HBV appears to be linked to psychosocial/behavioural factors. More effective screening/management of coinfection and metabolic syndrome, as well as strategies for smoking cessation, should be included in clinical follow-up.
Keywords: HIV; behaviour; hepatitis; liver disease; socioeconomy; urbanisation.
© 2025 The Author(s). Liver International published by John Wiley & Sons Ltd.
Conflict of interest statement
Anders Boyd reports speaker fees from Gilead Sciences. Dirk Posthouwer reports advisory board and speaker fees from Gilead Sciences. Marc Van der Valk reports grants or contracts and consulting fees from Gilead, ViiV Healthcare, and MSD to his institution. The other authors have no conflicts of interest to declare.
Figures
References
-
- Leumi S., Bigna J. J., Amougou M. A., Ngouo A., Nyaga U. F., and Noubiap J. J., “Global Burden of Hepatitis B Infection in People Living With Human Immunodeficiency Virus: A Systematic Review and Meta‐Analysis,” Clinical Infectious Diseases 71 (2020): 2799–2806. - PubMed
-
- Han W. M., Ueaphongsukkit T., Chattranukulchai P., et al., “Incident Liver Cirrhosis, Associated Factors, and Cardiovascular Disease Risks Among People Living With HIV: A Longitudinal Study,” Journal of Acquired Immune Deficiency Syndromes 86 (2021): 463–472. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
