

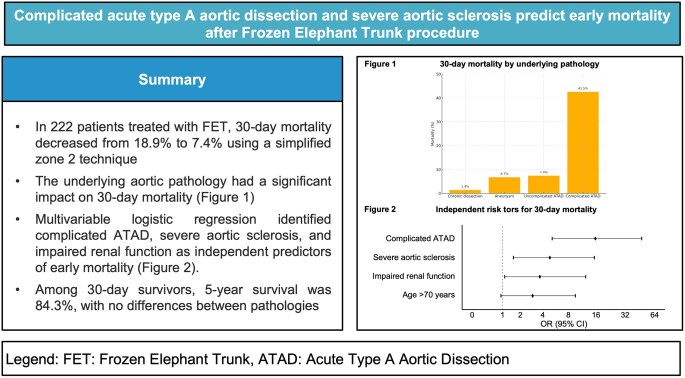
Complicated acute type A aortic dissection and severe aortic atherosclerosis predict early mortality after frozen elephant trunk procedure
- PMID: 40576437
- PMCID: PMC12270253
- DOI: 10.1093/ejcts/ezaf213
Complicated acute type A aortic dissection and severe aortic atherosclerosis predict early mortality after frozen elephant trunk procedure
Abstract
Objectives: To analyse risk factors for early mortality and long-term survival including secondary distal aortic interventions in patients undergoing frozen elephant trunk surgery.
Methods: A retrospective single-centre study was conducted, including all 222 patients who underwent frozen elephant trunk surgery between 2010 and 2022. We used multivariable regression analysis to detect risk factors for early mortality and Kaplan-Meier analysis for long-term survival and secondary interventions. We introduce the term 'complicated acute type A dissection' for those patients in whom the dissection was complicated by malperfusion syndrome, aortic rupture, pre-hospital intubation or resuscitation.
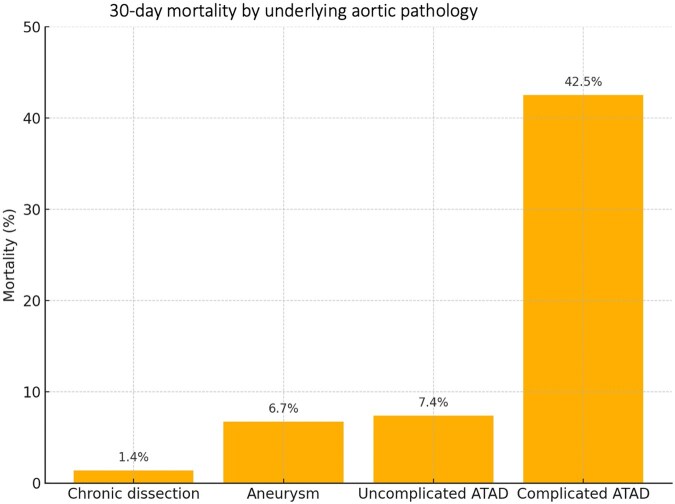
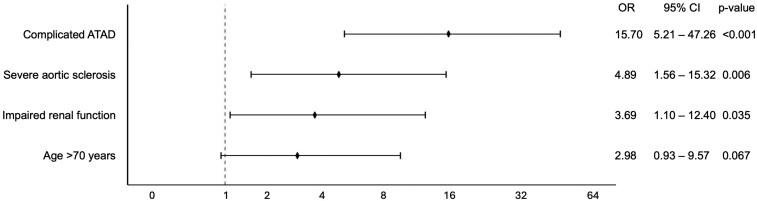
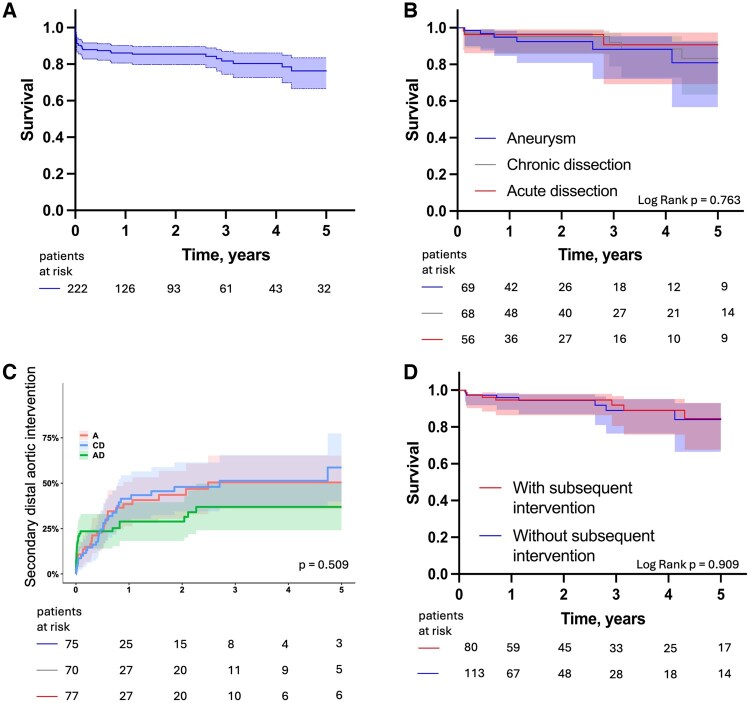
Results: Thirty-day mortality decreased significantly from 18.9% using the conventional zone 3 technique to 7.4% using a simplified zone 2 technique (P = 0.014). The aortic pathology had a significant impact on 30-day mortality: 1.4% in chronic dissection, 6.7% in aortic aneurysm, 7.4% in noncomplicated acute type A aortic dissection and 42.5% in complicated acute type A aortic dissection (P < 0.001). We identified complicated acute type A aortic dissection [odds ratio 15.7, confidence interval (CI) 5.2-47.3, P < 0.001], severe aortic atherosclerosis (odds ratio 4.9, CI 1.6-15.3, P = 0.006) and impaired renal function (odds ratio 3.7, CI 1.1-12.4, P = 0.035) as independent predictors of early mortality. Among 30-day survivors, 5-year survival was 84.3%, with no differences between pathologies. Secondary distal aortic interventions (37.4%) did not affect 5-year survival (P = 0.909).
Conclusions: Early mortality after frozen elephant trunk surgery is strongly driven by preoperative patient condition, particularly in the presence of complicated acute type A dissection. Once the early postoperative phase is overcome, long-term outcome is favourable across pathologies, regardless of secondary interventions. Careful patient selection and regular follow-up are crucial for optimizing outcomes.
Keywords: Aortic aneurysm; Aortic arch; Frozen elephant trunk; Type A aortic dissection.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Detter C, Demal TJ, Bax L et al. Simplified frozen elephant trunk technique for combined open and endovascular treatment of extensive aortic diseases. Eur J Cardiothorac Surg 2019;56:738–45. - PubMed
-
- Tokuda Y, Narita Y, Fujimoto K et al. Neurologic deficit after aortic arch replacement: the influence of the aortic atherosclerosis. Ann Thorac Surg 2019;108:107–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
