

Medullary Thyroid Cancer Risk and Mortality in Carriers of Incidentally Identified MEN2A RET Variants
- PMID: 40577012
- PMCID: PMC12205402
- DOI: 10.1001/jamanetworkopen.2025.17937
Medullary Thyroid Cancer Risk and Mortality in Carriers of Incidentally Identified MEN2A RET Variants
Erratum in
-
Error in Figure 1.JAMA Netw Open. 2025 Aug 1;8(8):e2528458. doi: 10.1001/jamanetworkopen.2025.28458. JAMA Netw Open. 2025. PMID: 40748643 Free PMC article. No abstract available.
Abstract
Importance: RET germline pathogenic variants cause multiple endocrine neoplasia type 2 (MEN2), which is associated with medullary thyroid cancer. With increasing incidental identification of these variants in asymptomatic individuals outside family screening, these individuals' risk of medullary thyroid cancer and all-cause mortality without intervention remain unknown in this context.
Objective: To evaluate the risk of medullary thyroid cancer and all-cause mortality in clinically unselected individuals with incidentally identified RET variants and assess whether the risk of medullary thyroid cancer differs from those with clinically ascertained RET variants.
Design, setting, and participants: This prospective cohort study of 383 914 unrelated individuals from the clinically unselected UK population (UK Biobank, recruited in 2006-2010, with follow-up to June 2023) and 122 640 unrelated individuals from a US health system (Geisinger MyCode cohort, recruited 2004-2020, with follow-up to October 2023) compared medullary thyroid cancer risk in these cohorts with 1078 individuals who were clinically ascertained with suspicion of MEN2 from a UK routine practice.
Exposures: RET germline pathogenic variants causing MEN2.
Main outcomes and measures: Frequency and the spectrum of pathogenic RET variants, risk of clinically present medullary thyroid cancer, and all-cause mortality without thyroidectomy were assessed using proportions with exact binomial 95% CIs and survival analysis adjusted for age at recruitment and sex.
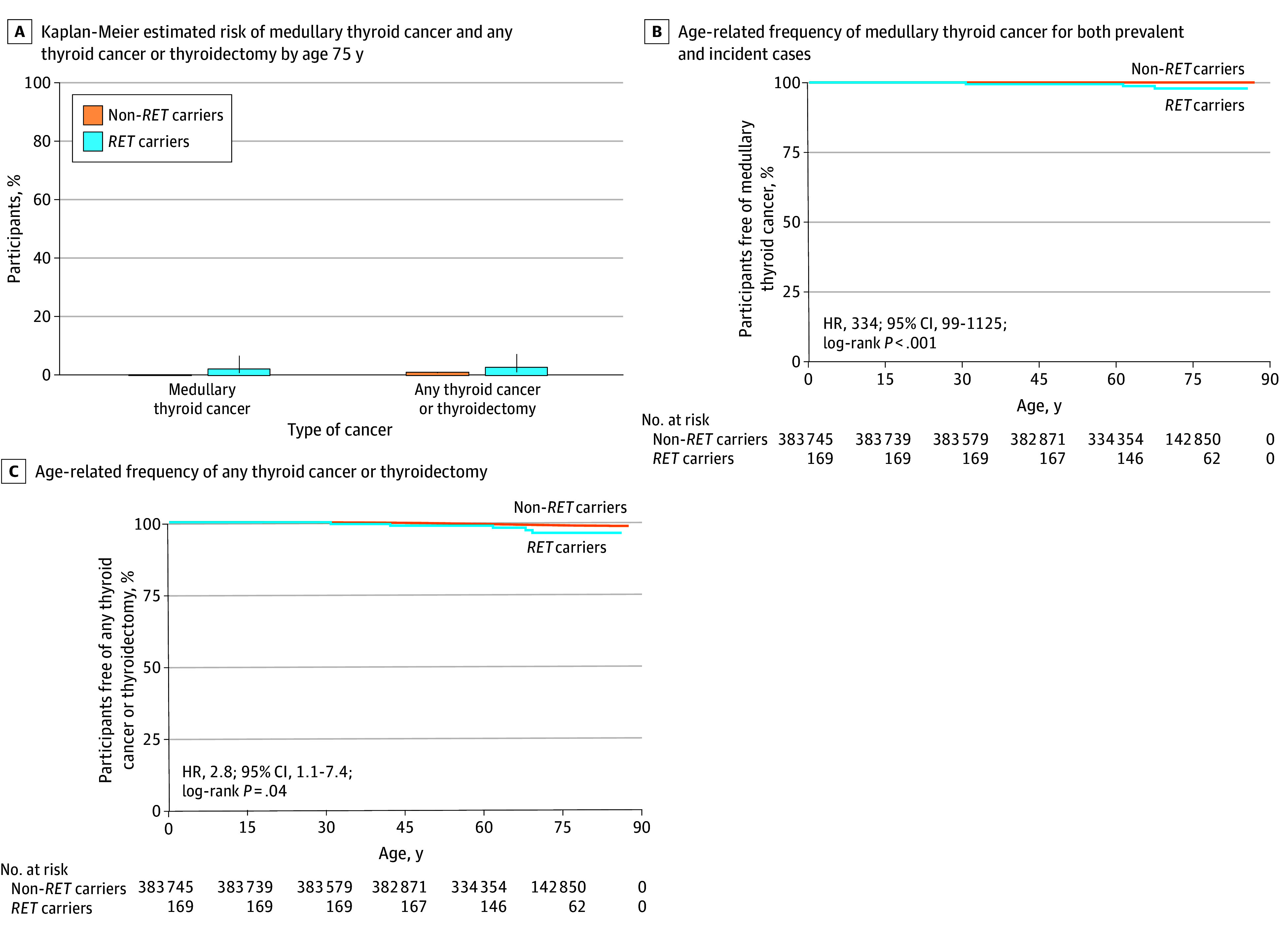
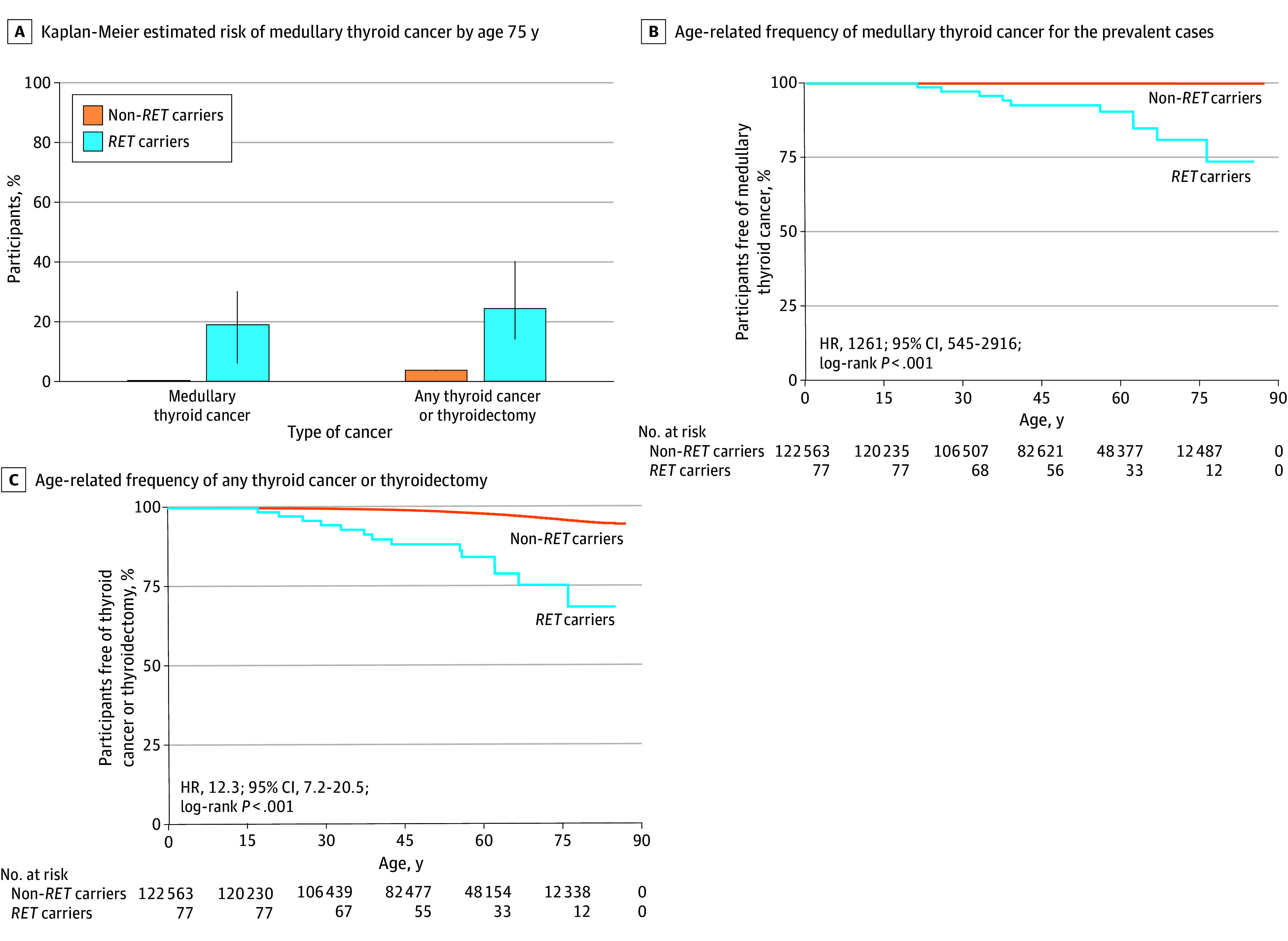
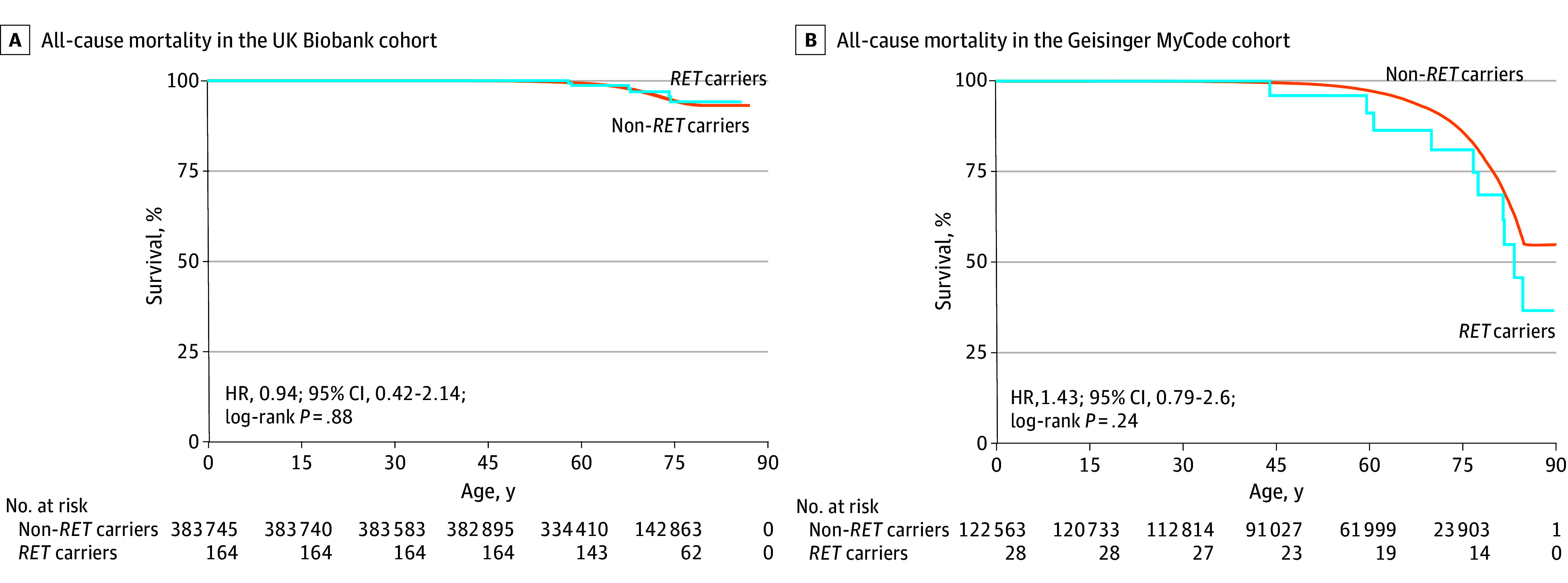
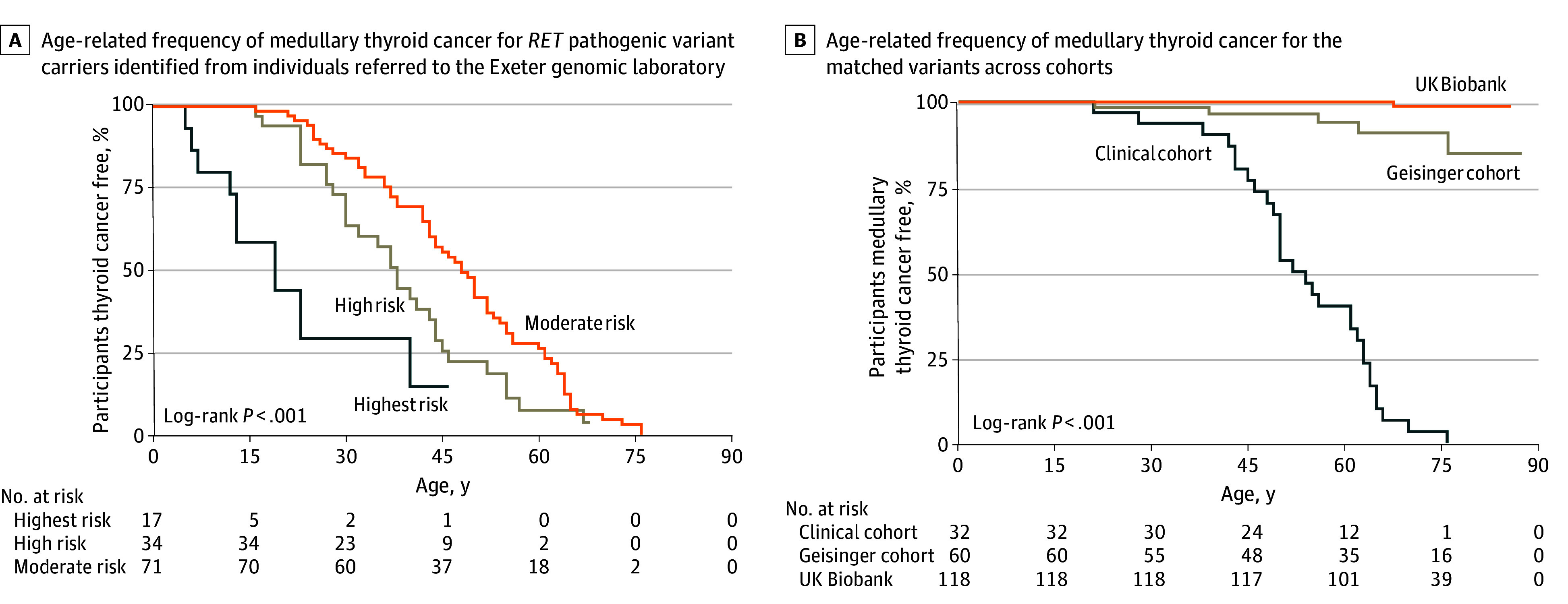
Results: In the UK Biobank, 169 unrelated individuals (mean [SD] age at recruitment, 57.0 [8.1] years; 94 male [55.6%]) had a pathogenic RET variant (prevalence, 0.04% [95% CI, 0.04%-0.05%]). In the US health system-based cohort, 77 unrelated individuals (mean [SD] age at recruitment, 56.2 [17.8] years; 45 female [58.4%]) had a pathogenic RET variant (prevalence, 0.06% [95% CI, 0.05%-0.78%]). The variants were predominantly from the moderate-risk category per American Thyroid Association guidelines (168 individuals [99.4%] and 75 individuals [94.8%], respectively). The Kaplan-Meier estimated medullary thyroid cancer risk by age 75 years in variant carriers in the UK population was 2.2% (95% CI, 0.7%-6.9) and 19.3% (95% CI, 6.4%-30.2%) in US health system cohort. These risks were significantly lower compared with the clinically ascertained cohort with the matched variants (95.7% [95% CI, 82.1%-99.7%]). In the UK Biobank, most variant carriers (166 [98.2%]) did not undergo thyroidectomy, and their all-cause mortality by age 75 years was similar to noncarriers (6.1% [95% CI, 2.7%-13.8%] vs 5.7% [95% CI, 5.6%-5.8%]), with consistent findings in the US health system cohort.
Conclusions and relevance: In this cohort study, moderate-risk RET variants were most common in incidental cases. The variants were associated with a substantially lower medullary thyroid cancer risk than clinically ascertained cases. This evidence addresses a current knowledge gap, enabling more informed clinical decision-making.
Conflict of interest statement
Figures
References
-
- Eng C, Plitt G. Multiple endocrine neoplasia type. In: Adam MP, Mirzaa GM, Pagon RA, eds. GeneReviews. University of Washington, Seattle;2023. Accessed February 7, 2025. https://www.ncbi.nlm.nih.gov/books/NBK1257/
-
- Torresan F, Censi S, Pennelli G, Galuppini F, Mian C, Iacobone M. Prophylactic and early thyroidectomy in RET germline mutation carriers in pediatric and adult population: long-term outcomes of a series of 63 patients. Cancers (Basel). 2022;14(24):6226. doi: 10.3390/cancers14246226 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
