

Survival benefit of radical prostatectomy in bone metastatic prostate cancer stratified by disease characteristics: A SEER-based retrospective analysis
- PMID: 40577265
- PMCID: PMC12204512
- DOI: 10.1371/journal.pone.0326429
Survival benefit of radical prostatectomy in bone metastatic prostate cancer stratified by disease characteristics: A SEER-based retrospective analysis
Abstract
Background: The role of radical prostatectomy (RP) in patients with newly diagnosed bone-metastatic prostate cancer (PCa) remains insufficiently explored.
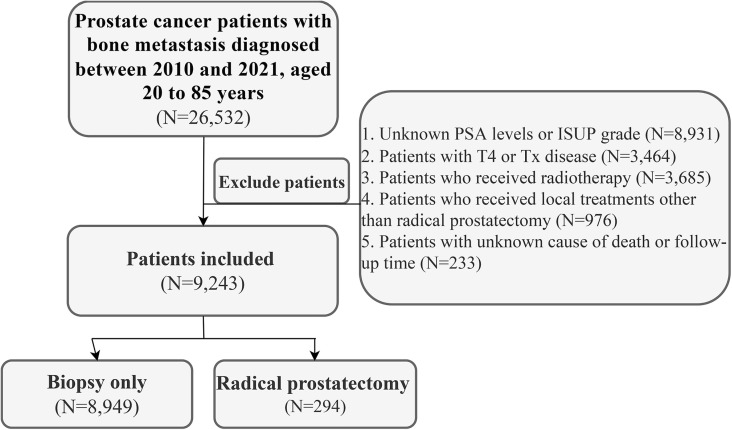
Patients and methods: Patients with newly diagnosed bone-metastatic PCa were retrospectively identified from the SEER-17 database and categorized into two groups based on local treatment: biopsy-only and RP. Notably, patients who had received radiotherapy were excluded due to the unavailability of radiotherapy target site details in the SEER database, which made it impossible to determine whether the radiotherapy was directed at metastatic lesions or the prostate. Kaplan-Meier methods were used to estimate cancer-specific survival (CSS) and overall survival (OS) between the two groups. Subgroup analyses stratified by T stage, N stage, PSA levels, and ISUP grade were conducted to assess the impact of disease characteristics on the efficacy of RP. A risk score incorporating these disease characteristics (T stage, N stage, PSA level, ISUP grade) was assigned to each patient, and risk-stratified subgroup analyses were performed to further evaluate the relationship between the efficacy of RP and overall disease characteristics.
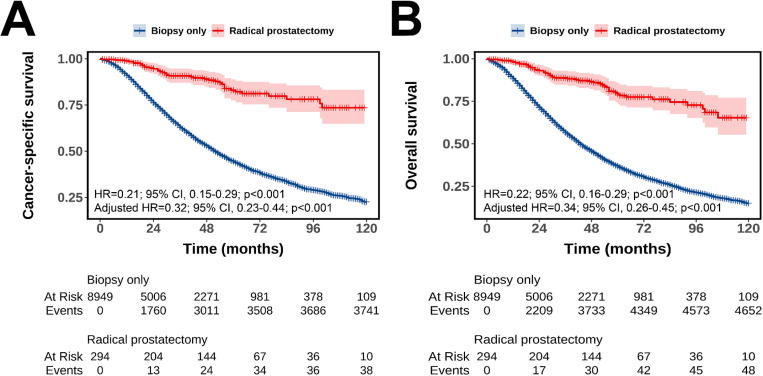
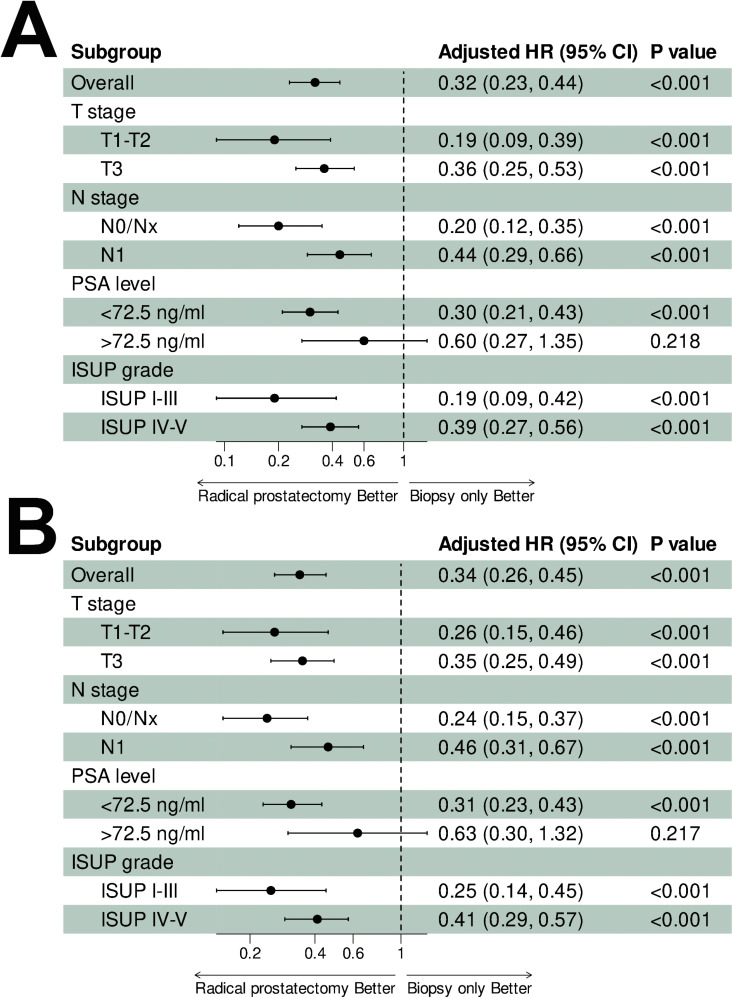
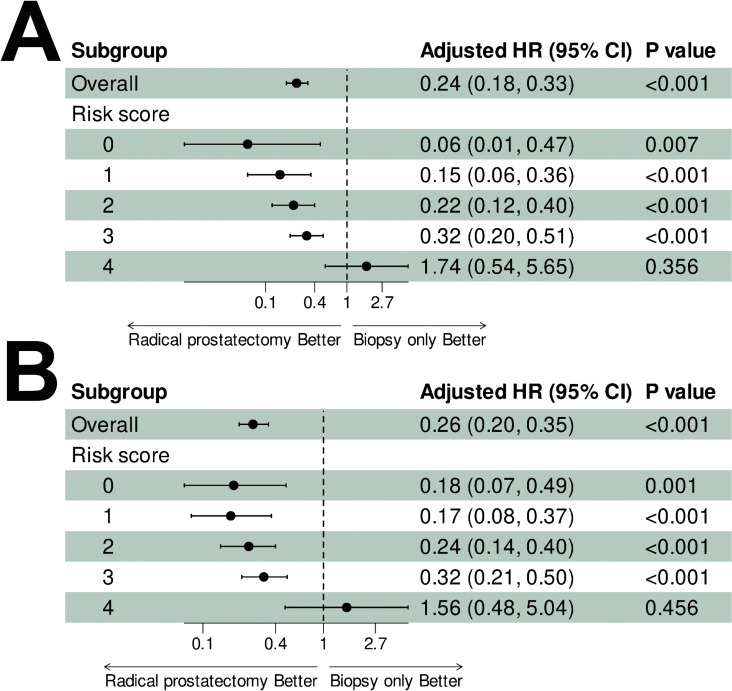
Results: A total of 9,243 patients were included in this study, of whom 8,949 (96.8%) underwent biopsy alone and 294 (3.2%) underwent RP. Patients who underwent RP had better CSS (adjusted HR = 0.32, 95% CI: 0.23-0.44, p < 0.001; 5-year CSS rate: 83.0% vs. 44.5%) and OS (adjusted HR = 0.34, 95% CI: 0.26-0.45, p < 0.001; 5-year OS rate: 79.2% vs. 36.9%) compared with patients who underwent biopsy alone. The survival benefit persisted across all subgroups but were attenuated in patients with more advanced stage (T3 and N1) and higher grades of disease (PSA > 72.5 ng/ml and ISUP grade IV-V). Risk score analysis revealed diminishing benefits with increasing scores. Significant survival benefits were observed for scores 0-3 (all adjusted HR < 1, p < 0.05), whereas no survival differences were detected at the highest risk score (CSS: adjusted HR = 1.74, 95% CI: 0.54-5.65, p = 0.356; OS: adjusted HR = 1.56, 95% CI: 0.48-5.04, p = 0.456).
Conclusion: Survival benefits of RP in de novo bone metastatic prostate cancer are modulated by disease characteristics, with attenuated effects in advanced/high-grade disease. Risk-stratified patient selection is critical, and prospective studies are needed to validate optimal candidacy for RP.
Copyright: © 2025 Zhang, Wang. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Brunckhorst O, Darraugh J, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024 Update. Part I: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol. 2024;86(2):148–63. doi: 10.1016/j.eururo.2024.03.027 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
