

Intra-Arterial Thrombolysis Following Endovascular Recanalization for Large Vessel Occlusion Stroke: A Systematic Review and Meta-Analysis
- PMID: 40577652
- PMCID: PMC12239893
- DOI: 10.1212/WNL.0000000000213842
Intra-Arterial Thrombolysis Following Endovascular Recanalization for Large Vessel Occlusion Stroke: A Systematic Review and Meta-Analysis
Abstract
Background and objectives: This systematic review and meta-analysis aims to evaluate the treatment effects of intra-arterial thrombolysis (IAT) after endovascular recanalization in patients with acute ischemic stroke (AIS) due to large vessel occlusion (LVO). Endovascular recanalization is the standard treatment for large vessel occlusion (LVO) stroke. Despite successful reperfusion after thrombectomy, fewer than half of the patients regain functional independence at 90 days, highlighting the potential role of impaired microcirculation in poor neurologic outcomes. The efficacy and safety of intra-arterial thrombolysis (IAT) after endovascular recanalization remains controversial. This systematic review and meta-analysis aims to evaluate the treatment effects of IAT after endovascular recanalization in patients with acute ischemic stroke (AIS) due to LVO.
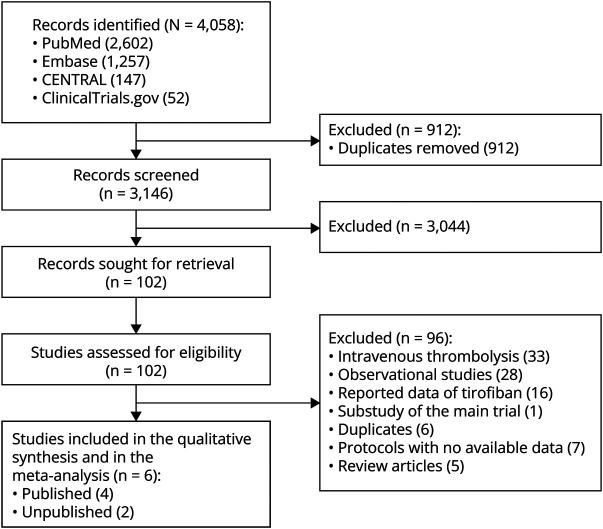
Methods: We conducted a study-level systematic review and meta-analysis based on PubMed, Embase, CENTRAL, and ClinicalTrials.gov from database inception to February 8, 2025. Only randomized controlled trials (RCTs) reporting the efficacy and safety of IAT after endovascular recanalization in large vessel occlusion stroke were included. The risk of bias of the included studies was assessed using the Risk of Bias 2 tool. The pooled data were analyzed using a random-effects meta-analysis. Our primary outcome was the proportion of patients with modified Rankin Scale (mRS) scores 0-1 at 90 days. Other outcomes included the proportion of patients with mRS scores 0-2 at 90 days, all-cause mortality at 90 days, and symptomatic intracranial hemorrhage and any intracranial hemorrhage within 48 hours. The study protocol was registered on PROSPERO (CRD42025639519).
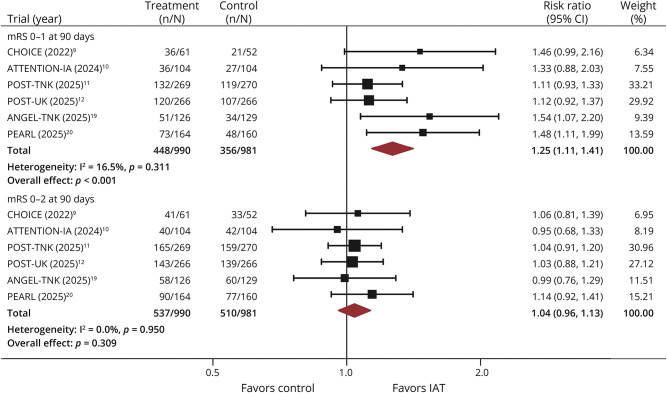
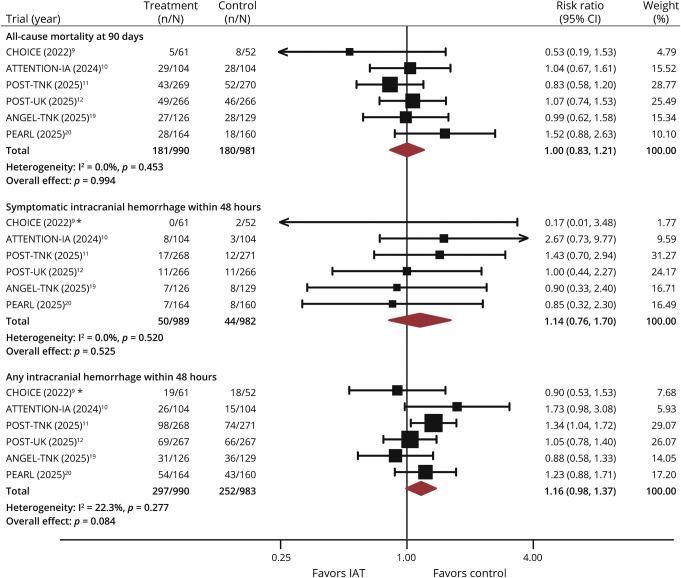
Results: A total of 6 RCTs with 1,985 initially enrolled patients were included in the analysis. A higher proportion of mRS scores 0-1 at 90 days was observed in the IAT group (risk ratio [RR] 1.25, 95% CI 1.11-1.41). No significant differences were found in the proportion of mRS scores 0-2 at 90 days (RR 1.04, 95% CI 0.96-1.13) between the groups. Regarding safety outcomes, 90-day all-cause mortality (RR 1.00, 95% CI 0.83-1.21), symptomatic intracranial hemorrhage (RR 1.14, 95% CI 0.76-1.70), and any intracranial hemorrhage (RR 1.16, 95% CI 0.98-1.37) were similar in the IAT group and control group.
Discussion: Among patients with AIS due to LVO, IAT after endovascular recanalization adds additional benefits to functional outcomes, with no increased risk of death or intracranial hemorrhage.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
Comment in
-
Should We Routinely Administer Intra-Arterial Thrombolysis After Endovascular Thrombectomy for Ischemic Stroke From Large Vessel Occlusion?Neurology. 2025 Aug 12;105(3):e213929. doi: 10.1212/WNL.0000000000213929. Epub 2025 Jun 27. Neurology. 2025. PMID: 40577653 No abstract available.
References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi: 10.1161/STR.0000000000000211 - DOI - PubMed
-
- Jiang X, Zhao Z, Zhang Y, Lai L. The safety and efficacy of endovascular treatment for patients with ASPECTS <6 in anterior circulation stroke: a meta-analysis and subgroup analysis by imaging techniques. J Stroke Cerebrovasc Dis. 2020;29(10):105122. doi: 10.1016/j.jstrokecerebrovasdis.2020.105122 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical