

Predictive accuracy of ophthalmic artery Doppler for pre-eclampsia: a systematic review
- PMID: 40578856
- PMCID: PMC12207145
- DOI: 10.1136/bmjopen-2024-094348
Predictive accuracy of ophthalmic artery Doppler for pre-eclampsia: a systematic review
Abstract
Objectives: This systematic review investigated available evidence on the stand-alone and incremental predictive performance of ophthalmic artery Doppler (OAD) for pre-eclampsia.
Design: Systematic review.
Data sources: We conducted a literature search from PubMed (Medline), the Cochrane CENTRAL, EMBASE and Scopus from inception to 8 April 2025.
Eligibility criteria: Studies eligible for inclusion were prospective or retrospective cohort studies, case-control studies or randomised controlled trials that reported on the predictive performance of OAD for pre-eclampsia in singleton pregnancies; and conducted in either high-income country (HIC) or low- and middle-income country (LMIC).
Data extraction and synthesis: Two reviewers independently screened and assessed articles for inclusion. One reviewer then extracted data using a standardised data extraction sheet, and any uncertainties were discussed with a second reviewer. The Prediction model Risk of Bias Assessment Tool was used for quality and risk of bias assessment. Findings were summarised and reported according to the Preferred Reporting Items for Systematic Review and Meta-Analyses statement and synthesised qualitatively.
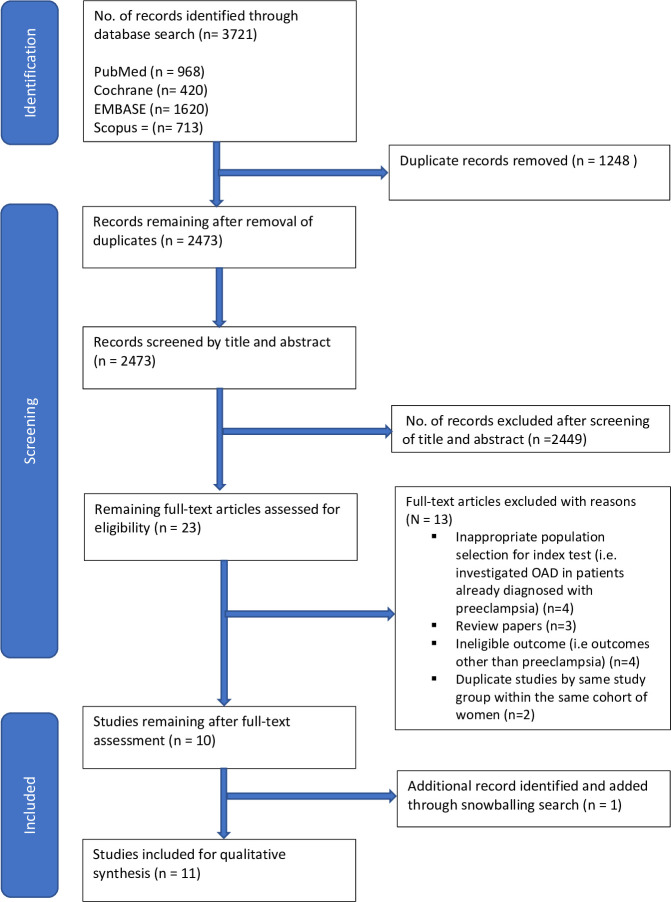
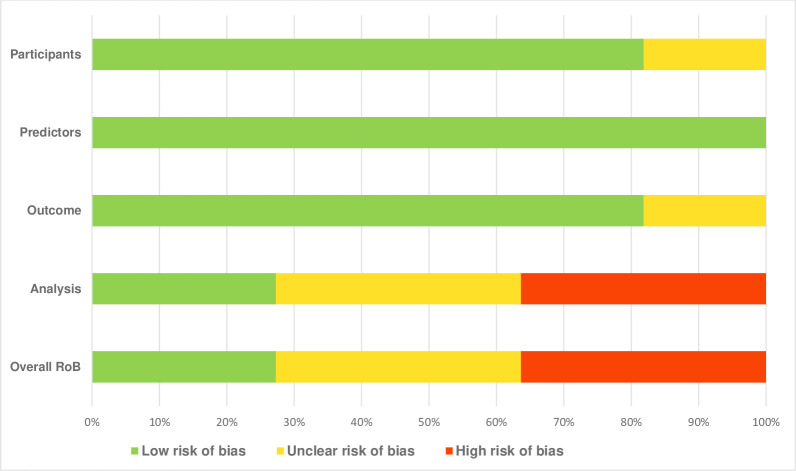
Results: We identified and included 11 observational studies (3 from HIC and 8 from LMICs) with a total of 12 150 singleton pregnancies, of which 517 (4.3%) were complicated by pre-eclampsia at end of follow-up. The included studies were of varied quality, with three at low risk of bias, four at unclear risk and four at high risk. No interventional study was identified. Three studies (27.3%) recruited high-risk pregnancies (defined according to the American College of Obstetricians and Gynecologists (ACOG) criteria as one or more of the following: chronic hypertension, personal or family history of pre-eclampsia, early (≤18 years) or late (≥40 years) first pregnancy, primipaternity, chronic kidney disease, increased body mass index >30 kg/m2, presence of diabetes mellitus prior to pregnancy, autoimmune disease and thrombophilia), while eight studies (72.7%) recruited undetermined risk pregnancies. Stand-alone performance of OAD (interpreted by area under the receiver operating curve at 95% CI) showed that in the first trimester, the peak systolic velocity (PSV) ratio demonstrated very good predictive ability (0.97, 95% CI 0.92 to 1.0) (n=1 study), and the second PSV (PSV2) demonstrated very good predictive ability (0.91, 95% CI 0.82 to 0.99) (n=1 study). Also, PSV2 demonstrated fair predictive ability (0.61, 95% CI 0.42 to 0.79; and 0.53, 95% CI 0.40 to 0.66) for early and late pre-eclampsia, respectively (n=1 study). In the second trimester, the PSV ratio demonstrated very good predictive ability (0.88, 95% CI 0.84 to 0.91) (n=1 study), and PSV2 demonstrated good predictive ability (0.73, 95% CI 0.66 to 0.81; and 0.76, 95% CI 0.71 to 0.81) for pre-eclampsia (n=2 studies). In the third trimester, the PSV ratio demonstrated good predictive ability (0.82, 95% CI 0.73 to 0.89; and 0.77, 95% CI 0.71 to 0.82) for preterm and term pre-eclampsia, respectively (n=1 study). Also, PSV2 demonstrated good predictive ability 0.70 (0.57 to 0.84) (n=1 study).Subsequently, in the second trimester, PSV ratio demonstrated better incremental predictive performance than uterine artery pulsatility index for preterm pre-eclampsia, when added to maternal factors and mean arterial pressure (MAP) (56.1%-80.2% vs 56.1%-74.8% detection rate (DR) at 10% FPR) (n=1 study). Also in the third trimester, adding PSV ratio to maternal factors and MAP was superior to soluble fms-like tyrosine kinase-1/placental growth factor ratio in predicting pre-eclampsia at <3 weeks after screening (96.7% vs 70% DR, p value 0.027) (n=1 study).
Conclusion: The ophthalmic artery PSV ratio and PSV2 are potentially useful ultrasound markers for pre-eclampsia prediction. Particularly in the second trimester, adding PSV ratio to maternal factors and MAP significantly improved the prediction of preterm pre-eclampsia. Given the burden of early and preterm pre-eclampsia in low-resource settings, OAD appears promising for pre-eclampsia screening in these settings where serum biomarkers may be expensive and inaccessible, and where uterine artery Doppler may not be technically feasible. However, the extent to which this novel marker is implemented in routine antenatal care should be guided by larger and sufficiently powered validation studies.
Prospero registration number: CRD42022324569.
Keywords: Maternal medicine; OBSTETRICS; Prenatal diagnosis; Ultrasound.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Accuracy of placental growth factor alone or in combination with soluble fms-like tyrosine kinase-1 or maternal factors in detecting preeclampsia in asymptomatic women in the second and third trimesters: a systematic review and meta-analysis.Am J Obstet Gynecol. 2023 Sep;229(3):222-247. doi: 10.1016/j.ajog.2023.03.032. Epub 2023 Mar 28. Am J Obstet Gynecol. 2023. PMID: 36990308
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Calcium supplementation commencing before or early in pregnancy, or food fortification with calcium, for preventing hypertensive disorders of pregnancy.Cochrane Database Syst Rev. 2017 Sep 26;9(9):CD011192. doi: 10.1002/14651858.CD011192.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2019 Sep 16;9:CD011192. doi: 10.1002/14651858.CD011192.pub3. PMID: 28949421 Free PMC article. Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous