

Washed up: the end of an era for adrenal incidentaloma CT
- PMID: 40579670
- PMCID: PMC12204974
- DOI: 10.1186/s13244-025-02015-4
Washed up: the end of an era for adrenal incidentaloma CT
Abstract
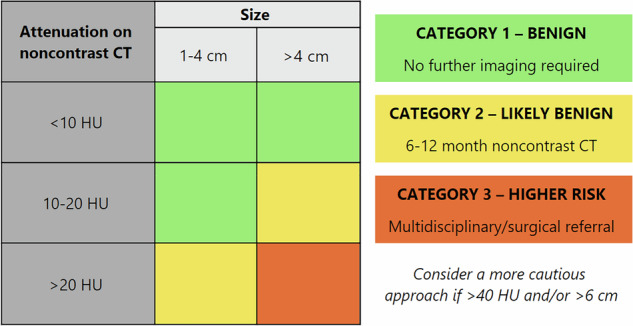
For over 20 years, the two key tenets of adrenal incidentaloma (AI) evaluation have been the upper threshold of 10 Hounsfield units (HU) on noncontrast CT (ncCT) to delineate benignity, and the utilisation of adrenal washout CT (AWCT) to evaluate those above this cutoff. In light of growing recent evidence that challenges these two traditional principles, as well as re-evaluation of the data that led to their acceptance, we conclude that neither of these mainstays of adrenal CT remains relevant in modern AI diagnostic workup. With an appropriate definition of an incidentaloma and endocrine assessment for the majority of adrenal lesions, our analysis establishes that the use of AWCT should be ceased in the assessment of AIs, and that a 20 HU attenuation threshold for lesions < 4 cm should replace the traditional 10 HU threshold to exclude malignancy in this patient population. We therefore propose new recommendations for the management of AIs based primarily on CT attenuation and lesion size on ncCT. CRITICAL RELEVANCE STATEMENT: Increasing the CT attenuation threshold to 20 HU for lesions < 4 cm and eliminating washout CT for true adrenal incidentalomas, together with recommendations for endocrine assessment, will significantly decrease the over-investigation of overwhelmingly benign adrenal lesions, whilst confidently excluding malignancy. KEY POINTS: True incidentalomas exclude current or prior extra-adrenal malignancy and clinically suspected adrenal disease. Adrenal washout CT was never proven in the malignancy-sparse true incidentaloma population. Hormonal correlation in parallel with < 20 HU and < 4 cm thresholds of homogeneous lesions on noncontrast CT excludes malignancy.
Keywords: Adrenal gland neoplasms; Adrenal incidentaloma; Tomography (x-ray computed).
© 2025. Crown.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
NIH state-of-the-science statement on management of the clinically inapparent adrenal mass ("incidentaloma").NIH Consens State Sci Statements. 2002 Feb 4-6;19(2):1-25. NIH Consens State Sci Statements. 2002. PMID: 14768652
-
A Study of Adrenal Incidentaloma-Related Hormonal Assays After First Integration of the Diagnosis Within Primary Healthcare.Diseases. 2025 May 26;13(6):169. doi: 10.3390/diseases13060169. Diseases. 2025. PMID: 40558580 Free PMC article.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.Health Technol Assess. 2006 Jun;10(18):iii-iv, xi-259. doi: 10.3310/hta10180. Health Technol Assess. 2006. PMID: 16729917
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature.Health Technol Assess. 2012 Dec;16(50):i-xvi, 1-159. doi: 10.3310/hta16500. Health Technol Assess. 2012. PMID: 23302507 Free PMC article.
References
-
- Caoili EM, Korobkin M, Francis IR et al (2002) Adrenal masses: characterization with combined unenhanced and delayed enhanced CT. Radiology 222:629–633. 10.1148/radiol.2223010766 - PubMed
-
- Mayo-Smith WW, Song JH, Boland GL et al (2017) Management of incidental adrenal masses: a white paper of the ACR Incidental Findings Committee. J Am Coll Radiol 14:1038–1044. 10.1016/j.jacr.2017.05.001 - PubMed
-
- Fassnacht M, Tsagarakis S, Terzolo M (2023) European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 189:G1–G42. 10.1093/ejendo/lvad066 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
