

Catastrophic health expenditure, social protection coverage, and financial coping strategies in adults with symptoms of chronic respiratory diseases in Kenya: a cross-sectional study
- PMID: 40580995
- PMCID: PMC12208783
- DOI: 10.1016/S2214-109X(25)00061-0
Catastrophic health expenditure, social protection coverage, and financial coping strategies in adults with symptoms of chronic respiratory diseases in Kenya: a cross-sectional study
Abstract
Background: Despite the socioeconomic consequences of an increasing burden of chronic respiratory diseases, there is little evidence on the incidence and determinants of catastrophic health expenditure (CHE) in people with chronic respiratory disease symptoms in Kenya. We aimed to generate this evidence by collecting data on medical and non-medical costs, lost income, social protection coverage, and financial coping strategies for such people in Kenya.
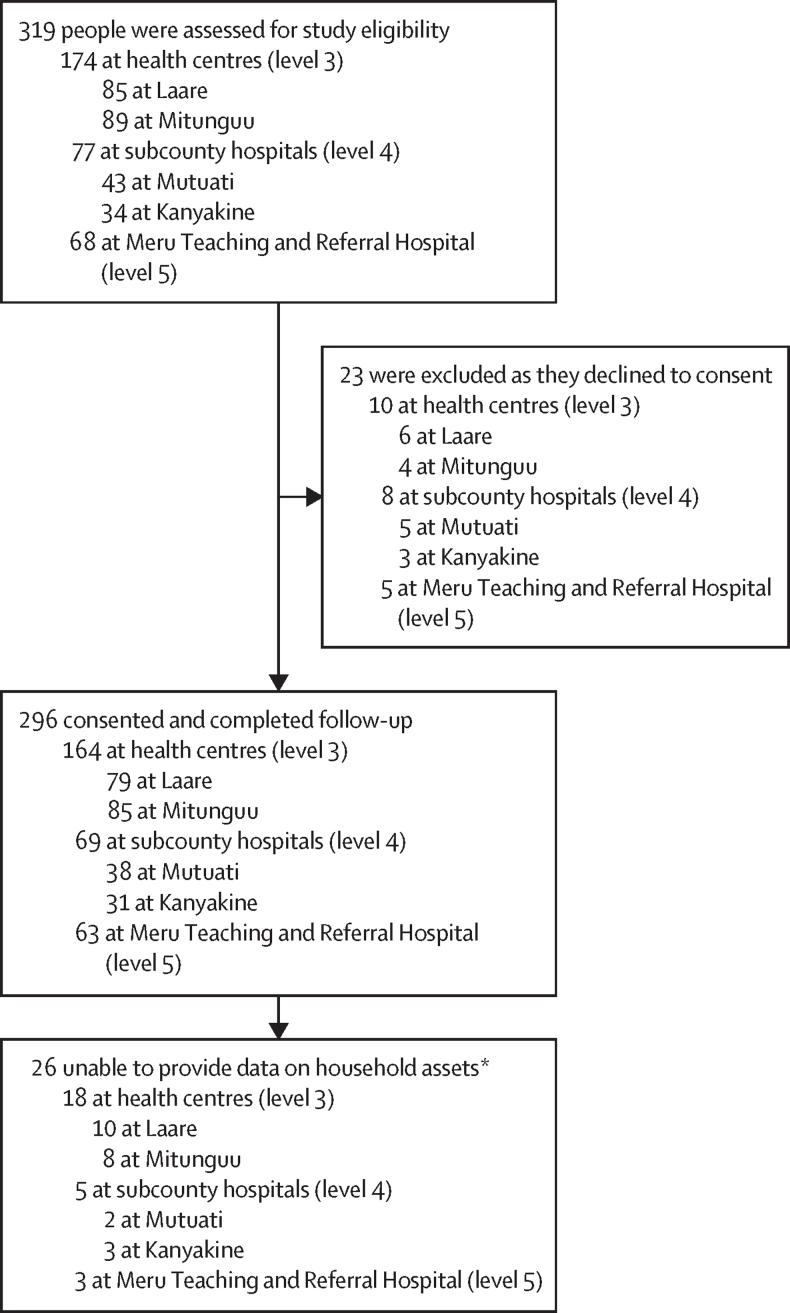
Methods: We conducted a cross-sectional survey of consecutively recruited adults seeking care for chronic respiratory disease symptoms at five public health-care facilities in Meru County, Kenya, between Sept 5, 2019, and Oct 1, 2020. Patient costs, National Health Insurance Fund (NHIF) coverage, financial coping strategies, and sociodemographic and clinical data were collected from surveys and medical records. The main study outcomes were the incidence of, and social and health factors associated with, CHE in this cohort. CHE incidence was calculated through the WHO threshold of direct out-of-pocket costs being greater than 10% of a household's monthly total expenditure. Multivariable logistic regression analyses generated adjusted odds ratios (aORs) with 95% CIs of health and social factors associated with CHE, including age, sex, education level, tobacco use, income, being accompanied, poverty level (with the first quintile being the richest to the fifth quintile being the poorest), NHIF usage, coping strategies, final diagnosis, and health system level at which they were seeking care.
Findings: Of 319 eligible people invited, 296 (93%) consented to participate and completed surveys. Mean total cost was 1062 Kenyan shillings (KES; 95% CI 896-1228; US$9·1), of which 40·0% was due to direct non-medical costs (KES 425, 95% CI 361-489; $3·7), 36·7% to direct out-of-pocket medical costs (KES 390, 324-456; $3·1), and 23·3% to lost income (KES 247, 153-341, $2·1). 212 (72%) of 296 participants did not have NHIF, 282 (95%) of 296 used coping strategies during care-seeking, and 59 (20%) of 296 were accompanied by a carer during health-care seeking. 76 (26%) of 296 participants had CHE. CHE was associated with being aged 30-44 years old (aOR 2·6, 95% CI 1·3-5·3, p=0·010), being female (1·8, 1·3-2·7, p=0·0021), having higher than secondary school education (1·6, 1·1-2·3, p=0·0083), being accompanied during health-care-seeking visits (3·2, 1·7-5·9, p<0·0001), belonging to the second poverty quintile (2·0, 1·9-2·1, p<0·0001), and seeking care from subcounty hospitals (9·7, 9·6-9·8, p<0·0001) and county hospitals (25·1, 15·7-40·2, p<0·0001).
Interpretation: These findings suggest a sizeable burden of CHE in people seeking care for chronic respiratory disease symptoms in Meru County in Kenya, driven by socioeconomic and sex inequalities and impaired access to health care and social protection.
Funding: UK-Aid, UK National Institute for Health and Care Research, and UK Research and Innovation.
Copyright © 2025 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TW is supported by grants from the Wellcome Trust, UK (209075/Z/17/Z); the Medical Research Council, Department for International Development, and Wellcome Trust (Joint Global Health Trials, MR/V004832/1); the Medical Research Council (PHIND, MR/Y503216/1); and the Medical Research Foundation (Dorothy Temple Cross International Collaboration Research Grant, MRF-131–0006-RG-KHOS-C0942) and receives consultancy fees from WHO for ad hoc consultancy related to tuberculosis. MT is a trustee on a registered UK charity called National Friendship Fund but does not receive fees or honoraria for this role. All other authors declare no competing interests.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Unconditional cash transfers for reducing poverty and vulnerabilities: effect on use of health services and health outcomes in low- and middle-income countries.Cochrane Database Syst Rev. 2017 Nov 15;11(11):CD011135. doi: 10.1002/14651858.CD011135.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2022 Mar 29;3:CD011135. doi: 10.1002/14651858.CD011135.pub3. PMID: 29139110 Free PMC article. Updated.
-
Catastrophic Health Expenditures for In-State and Out-of-State Abortion Care.JAMA Netw Open. 2024 Nov 4;7(11):e2444146. doi: 10.1001/jamanetworkopen.2024.44146. JAMA Netw Open. 2024. PMID: 39514227 Free PMC article.
Cited by
-
The COVID-19 Pandemic Economic Implications in Iran: A National Survey Assessing Catastrophic Health Expenditures.Interdiscip Perspect Infect Dis. 2025 Jul 23;2025:8854646. doi: 10.1155/ipid/8854646. eCollection 2025. Interdiscip Perspect Infect Dis. 2025. PMID: 40741354 Free PMC article.
References
-
- WHO Noncommunicable diseases. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-disease...
-
- WHO Monitoring health for the SDGs. https://www.who.int/health-topics/sustainable-development-goals#tab=tab_2
-
- Lagomarsino G, Garabrant A, Adyas A, Muga R, Otoo N. Moving towards universal health coverage: health insurance reforms in nine developing countries in Africa and Asia. Lancet. 2012;380:933–943. - PubMed
-
- Kenyan Ministry of Health National Strategic Plan for Tuberculosis, Leprosy and Lung Health, 2015–2018. 2014. https://nltp.co.ke/wp-content/uploads/2020/10/M-and-E-plan-2015–2018.pdf
-
- Kenyan Government. Constitution of Kenya. 2010.
MeSH terms
LinkOut - more resources
Full Text Sources
