

Acquired neuropathology and its associations with key patterns of placental pathology
- PMID: 40581648
- PMCID: PMC12205522
- DOI: 10.1186/s40478-025-02065-1
Acquired neuropathology and its associations with key patterns of placental pathology
Abstract
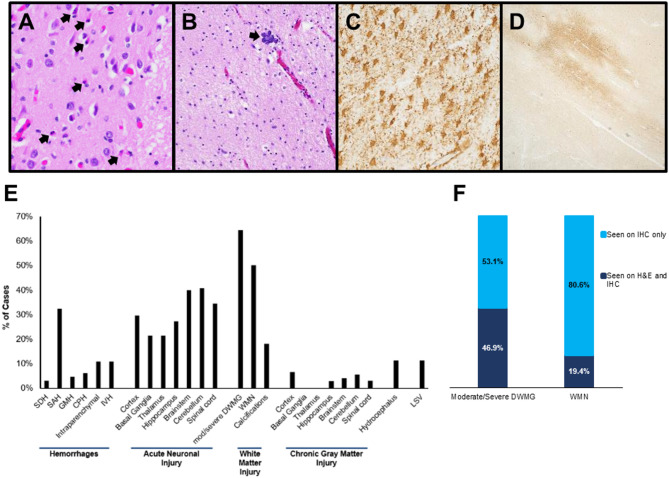
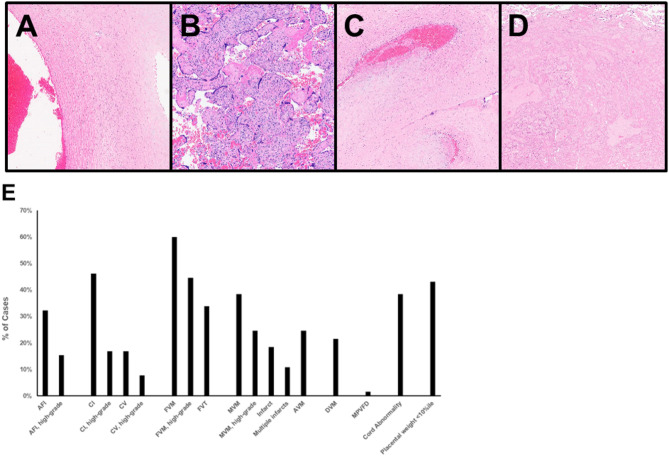
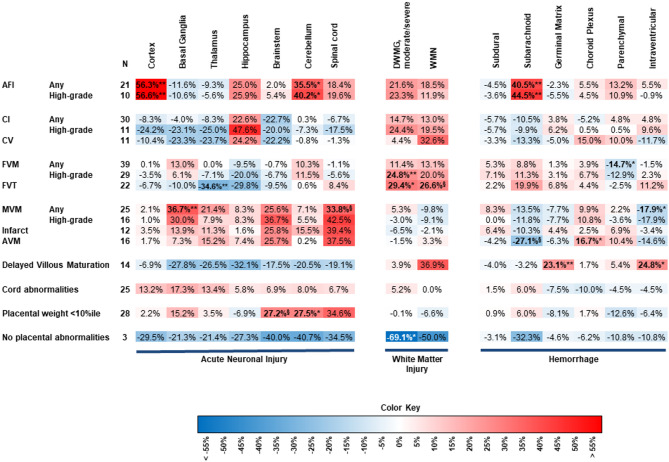
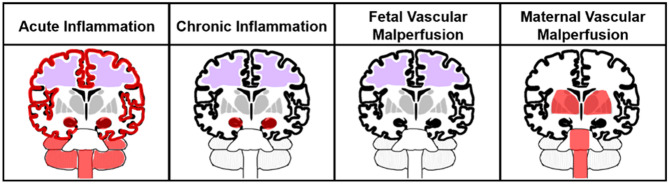
Perinatal brain injury is a major cause of neurodevelopmental disability worldwide. Placental pathology has been implicated as a likely cause of injury to the developing central nervous system (CNS). This study aims to elucidate the associations of multiple placental pathologies and CNS injury, including more subtle brain pathologies associated with adverse neurologic outcomes. Sixty-five subjects that underwent complete post-mortem neuropathologic examination and placental examination were selected for inclusion. Gross images, autopsy reports, and histologic sections from the CNS and placenta underwent blinded reviewed by experts in perinatal neuropathology and placental pathology, respectively. Immunostains useful in highlighting CNS lesions not apparent on routine histologic sections were performed. Placental pathology was classified according to the Amsterdam criteria, and all placental and CNS abnormalities were documented. A previously undescribed association between white matter injury and fetal vascular malperfusion was seen, likely due to improved detection of injury on immunohistochemical stains. Amniotic fluid infection was associated with acute neuronal injury in the cortex and cerebellum as well as subarachnoid hemorrhage. Hippocampal injury had the strongest association with high-grade chronic inflammation, and maternal vascular malperfusion showed higher relative frequencies of acute neuronal injury in the basal ganglia, brainstem, and spinal cord. To our knowledge, this is the first study to standardize placental pathology according to the Amsterdam consensus criteria, separate out injury across multiple CNS regions with independent assessment of these regions, and to utilize immunohistochemistry to improve detection of white matter injury. Different patterns of placental pathology were associated with different types of CNS injury, indicating neuronal injury and white matter injury may be influenced by distinct placental pathologies. Elucidating the placental contributions to these acquired CNS pathologies in stillborns is crucial for understanding long-term adverse neurodevelopmental outcomes associated with perinatal brain injury.
Keywords: Amsterdam criteria; Brain; Central nervous system; Injury; Neuropathology; Perinatal; Placenta; Stillbirth.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was granted exemption by the Children’s Hospital of Philadelphia Institutional Review Board Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Placental lesions in small for gestational age fetuses with and without clinical features of fetal growth restriction: a secondary analysis of the Doppler Ratio In fetal Growth restriction Intervention Trial At (near) Term (DRIGITAT) study.Am J Obstet Gynecol. 2025 May 30:S0002-9378(25)00349-7. doi: 10.1016/j.ajog.2025.05.022. Online ahead of print. Am J Obstet Gynecol. 2025. PMID: 40451449
-
Placental fetal vascular malperfusion, neonatal neurologic morbidity, and infant neurodevelopmental outcomes: a systematic review and meta-analysis.Am J Obstet Gynecol. 2023 Dec;229(6):632-640.e2. doi: 10.1016/j.ajog.2023.06.014. Epub 2023 Jun 12. Am J Obstet Gynecol. 2023. PMID: 37315755
-
Multiple-micronutrient supplementation for women during pregnancy.Cochrane Database Syst Rev. 2017 Apr 13;4(4):CD004905. doi: 10.1002/14651858.CD004905.pub5. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2019 Mar 14;3:CD004905. doi: 10.1002/14651858.CD004905.pub6. PMID: 28407219 Free PMC article. Updated.
-
Placental histopathology after SARS-CoV-2 infection in pregnancy: a systematic review and meta-analysis.Am J Obstet Gynecol MFM. 2021 Nov;3(6):100468. doi: 10.1016/j.ajogmf.2021.100468. Epub 2021 Aug 21. Am J Obstet Gynecol MFM. 2021. PMID: 34425296 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Anjari M, Counsell SJ, Srinivasan L, Allsop JM, Hajnal JV, Rutherford MA et al (2009) The association of lung disease with cerebral white matter abnormalities in preterm infants. Pediatrics 124(1):268–276. 10.1542/peds.2008-1294 - PubMed
-
- Burke C, Gobe G (2005) Pontosubicular apoptosis (necrosis) in human neonates with intrauterine growth retardation and placental infarction. Virchows Arch 446(6):640–645. 10.1007/s00428-005-1251-1 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
