

A comparative study of collagen morphology and joint strength in anterior cruciate ligament repair and reconstruction models in rabbits
- PMID: 40584110
- PMCID: PMC12205225
- DOI: 10.14202/vetworld.2025.1313-1321
A comparative study of collagen morphology and joint strength in anterior cruciate ligament repair and reconstruction models in rabbits
Abstract
Background and aim: Anterior cruciate ligament (ACL) repair offers several theoretical advantages over reconstruction, including preservation of native proprioception and reduced donor-site morbidity. However, the current experimental models are predominantly limited to ACL reconstruction, leaving a critical gap in ACL repair research. This study introduces a novel rabbit model to evaluate osteointegration and mechanical strength at the tendon/ligament-bone interface following ACL repair and reconstruction.
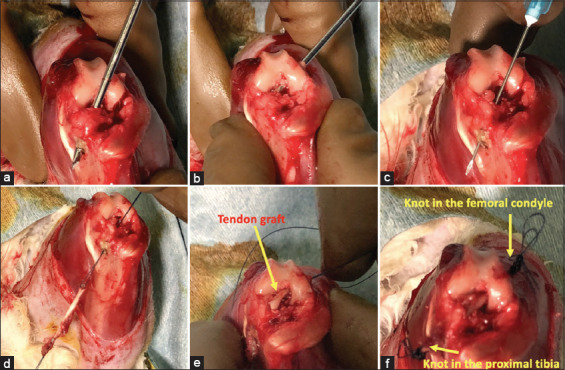
Materials and methods: Six male New Zealand White rabbits (Oryctolagus cuniculus), aged 90 ± 0 days and weighing 2.50 ± 0.20 kg, were randomly assigned to two groups: ACL reconstruction (n = 3) using the extensor digitorum longus tendon graft and ACL repair (n = 3) using the Krackow suture technique at the femoral attachment. Specimens were collected 6 weeks postoperatively for histological evaluation of Sharpey's-like fibers, immunohistochemical analysis of types I and III collagen, and biomechanical tensile testing.
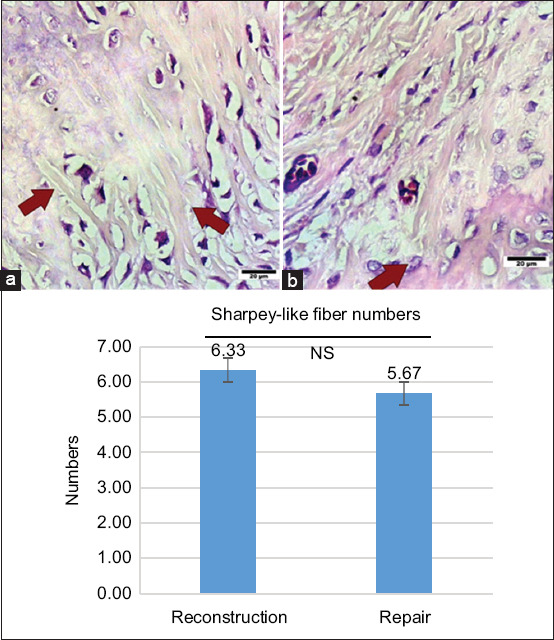
Results: All surgical procedures were completed without complications. Histological analysis showed greater numbers of Sharpey's-like fibers in the reconstruction group (6.33 ± 0.58%) compared to the repair group (5.67 ± 1.6%), though not statistically significant (p > 0.05). Type I collagen fibers were significantly longer in the reconstruction group in both longitudinal (3.10 ± 0.05 μm vs. 2.97 ± 0.04 μm) and transverse (1.94 ± 0.09 μm vs. 1.81 ± 0.05 μm) dimensions (p < 0.05). Type III collagen dimensions did not differ significantly. The mean tensile failure load was higher in the reconstruction group (105.96 ± 63.37 N) than in the repair group (62.56 ± 20.11 N), though this difference was not statistically significant (p > 0.05).
Conclusion: This study establishes a reproducible and cost-effective ACL repair model in rabbits and confirms that tendon-bone osteointegration occurs in both ACL repair and reconstruction. Superior biomechanical strength and enhanced type I collagen integration in the reconstruction group underscore current clinical outcomes favoring reconstruction. This model offers a valuable platform for exploring biological augmentation strategies to enhance ACL repair efficacy.
Keywords: anterior cruciate ligament repair; biomechanics; osteointegration; rabbit model; type I collagen.
Copyright: © Yanuar, et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





Similar articles
-
Bioabsorbable versus metallic interference screws for graft fixation in anterior cruciate ligament reconstruction.Cochrane Database Syst Rev. 2016 Jul 24;7(7):CD009772. doi: 10.1002/14651858.CD009772.pub2. Cochrane Database Syst Rev. 2016. PMID: 27450741 Free PMC article.
-
Surgical versus conservative interventions for treating anterior cruciate ligament injuries.Cochrane Database Syst Rev. 2016 Apr 3;4(4):CD011166. doi: 10.1002/14651858.CD011166.pub2. Cochrane Database Syst Rev. 2016. PMID: 27039329 Free PMC article.
-
What Factors Influence the Biomechanical Properties of Allograft Tissue for ACL Reconstruction? A Systematic Review.Clin Orthop Relat Res. 2017 Oct;475(10):2412-2426. doi: 10.1007/s11999-017-5330-9. Clin Orthop Relat Res. 2017. PMID: 28353048 Free PMC article.
-
Transportal versus all-inside techniques of anterior cruciate ligament reconstruction: a systematic review.J Orthop Surg Res. 2021 Dec 23;16(1):734. doi: 10.1186/s13018-021-02872-x. J Orthop Surg Res. 2021. PMID: 34949188 Free PMC article.
-
The Effect of Lateral Extra-articular Tenodesis on Anterior Cruciate Ligament Graft Forces and Knee Stability Compared With Slope Reduction Osteotomy in the Setting of Increased Posterior Tibial Slope.Am J Sports Med. 2025 Jul;53(8):1912-1920. doi: 10.1177/03635465251338236. Epub 2025 May 21. Am J Sports Med. 2025. PMID: 40396207
References
-
- LaBella C.R, Hennrikus W, Hewett T.E Council on Sports Medicine and Fitness. and Section on Orthopaedics. Anterior cruciate ligament injuries:Diagnosis, treatment, and prevention. Pediatrics. 2014;133(5):e1437–e1450. - PubMed
-
- Tsuda E, Okamura Y, Otsuka H, Komatsu T, Tokuya S. Direct evidence of the anterior cruciate ligament-hamstring reflex arc in humans. Am. J. Sports Med. 2001;29((1)):83–87. - PubMed
-
- Kapreli E, Athanasopoulos S, Gliatis J, Papathanasiou M, Peeters R, Strimpakos N, Hecke P.V, Gouliamos A, Sunaert S. Anterior cruciate ligament deficiency causes brain plasticity:A functional MRI study. Am. J. Sports Med. 2009;37((12)):2419–2426. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous