

Application of enhanced recovery after surgery in perioperative care of infants and children with Hirschsprung disease
- PMID: 40584501
- PMCID: PMC12188570
- DOI: 10.4240/wjgs.v17.i6.105739
Application of enhanced recovery after surgery in perioperative care of infants and children with Hirschsprung disease
Abstract
Background: Enhanced recovery after surgery (ERAS) represents an innovative, protocol-driven perioperative care program designed to optimize patient outcomes. However, its application and efficacy in infants and children with Hirschsprung disease (HD) remain underexplored.
Aim: To delve into the impact of ERAS on perioperative recovery and the overall medical experience in HD infants and children.
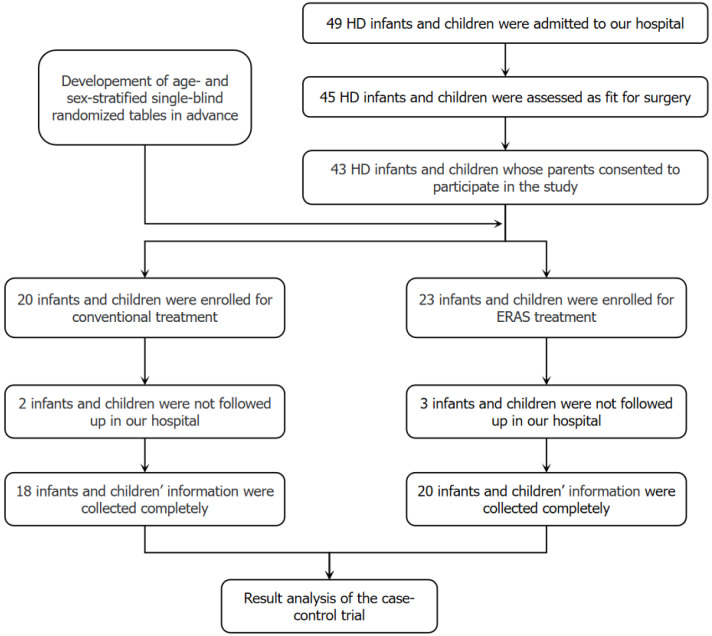
Methods: Thirty-eight infants and children with HD who received the Soave surgical procedure were enrolled in this case-control study. According to age- and sex-stratified single-blind randomized tables, 20 cases received ERAS treatment (ERAS group) and 18 cases received conventional treatment (control group). The two treatments were then compared in terms of perioperative recovery and medical experience.
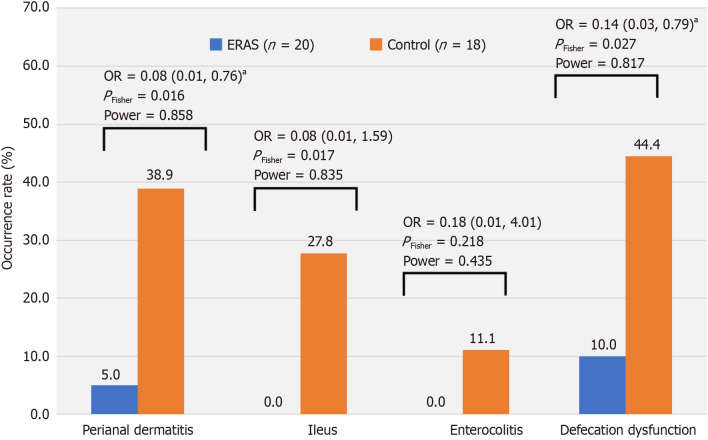
Results: Significant differences were observed in pain scores at awakening (4.2 ± 1.3 vs 5.2 ± 1.2, t = 2.516, P = 0.017) and pain duration (85.69 ± 7.46 hours vs 67.00 ± 8.56 hours, t = 7.139, P < 0.001) between the ERAS and control group. The recovery of bowel movement was earlier in the ERAS group than in the control group (borborygmus time: 33.63 ± 9.83 hours vs 44.69 ± 16.85 hours, t = 2.501, P = 0.017; feeding time: 36.63 ± 9.55 hours vs 49.36 ± 16.99 hours, t = 2.884, P = 0.007; anal catheter indwelling time: 75.83 ± 13.80 hours vs 93.36 ± 20.65 hours, t = 3.104, P = 0.004), and fever duration (40.73 ± 14.42 hours vs 52.63 ± 18.69 hours, t = 2.211, P = 0.034). In the ERAS group, hospital stay was shorter (7.5 ± 0.9 days vs 8.3 ± 1.2 days) and the cost was lower (14203 ± 2381 yuan vs 16847 ± 3558 yuan). During the 1-month follow-up period, of the multiple postoperative complications observed, the occurrence of perianal dermatitis (P Fisher = 0.016) and defecation dysfunction (P Fisher = 0.027) were lower in the ERAS group than in the control group.
Conclusion: The ERAS protocol has the potential to profoundly enhance postoperative recovery and significantly elevate the overall comfort and quality of the medical experience, making it an indispensable approach that warrants widespread adoption. Continuous refinement through evidence-based practices is anticipated to further optimize its efficacy.
Keywords: Complications; Enhanced recovery after surgery; Hirschsprung disease; Infant and children; Outcome; Perioperative period.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
Similar articles
-
Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults.Cochrane Database Syst Rev. 2018 Jun 4;6(6):CD009642. doi: 10.1002/14651858.CD009642.pub3. Cochrane Database Syst Rev. 2018. PMID: 29864216 Free PMC article.
-
Application of Enhanced Recovery after Surgery in the Perioperative Period for Elderly Patients with Lung Cancer.JSLS. 2024 Jul-Sep;28(3):e2024.00037. doi: 10.4293/JSLS.2024.00037. Epub 2025 Jan 10. JSLS. 2024. PMID: 39801728 Free PMC article. Clinical Trial.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Chewing gum for enhancing early recovery of bowel function after caesarean section.Cochrane Database Syst Rev. 2016 Oct 17;10(10):CD011562. doi: 10.1002/14651858.CD011562.pub2. Cochrane Database Syst Rev. 2016. PMID: 27747876 Free PMC article.
-
Efficacy of nursing interventions based on the enhanced recovery after surgery (ERAS) in patients with lumbar disc herniation.Sci Rep. 2025 Jul 1;15(1):21947. doi: 10.1038/s41598-025-01116-w. Sci Rep. 2025. PMID: 40592924 Free PMC article.
References
LinkOut - more resources
Full Text Sources
