

Real-world utilization of Cenobamate as adjunct therapy in office-based neurology: practical tips and insights for titration
- PMID: 40584530
- PMCID: PMC12202365
- DOI: 10.3389/fneur.2025.1558614
Real-world utilization of Cenobamate as adjunct therapy in office-based neurology: practical tips and insights for titration
Abstract
Introduction: Epilepsy poses significant management challenges, particularly in patients with refractory epilepsy where conventional antiseizure medications (ASMs) are ineffective. Cenobamate (CNB), a recently approved third-generation ASM, has shown unprecedented efficacy as an adjunctive therapy in clinic-based practice. However, to date, its use by office-based neurologists in Germany remains relatively limited. One reason for this is its perceived complexity and false perception as a medication of last resort. This study focuses on the logistics of German care pathways, CNB titration, and ASM combinations in a first cohort of office-based outpatients. It also gives a glimpse into which ASMs are being used in the office-based setting in comparison to population and clinic-based data sources.
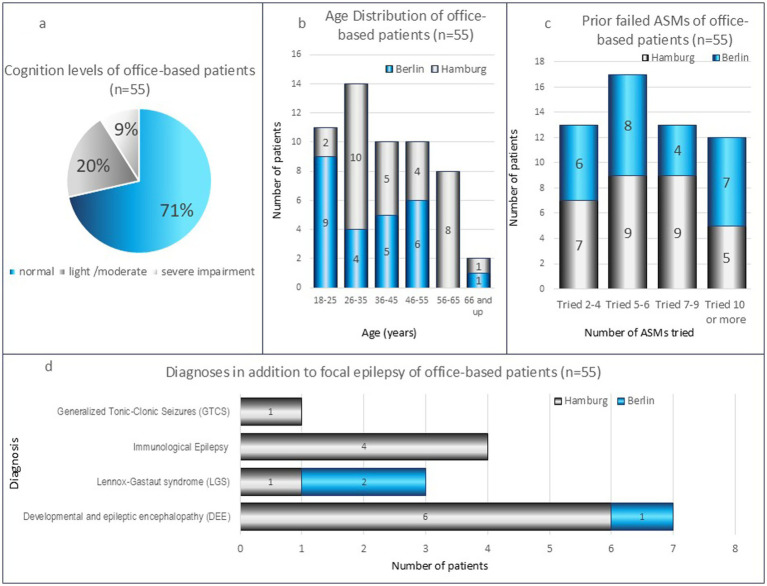
Methods: The cohort comprised 55 patients from two office-based outpatient practices (Niedergelassene) in Berlin (n = 25) and Hamburg (n = 30). All patients had a history of refractory epilepsy despite optimal treatment with existing ASMs. Patients were initiated on CNB from the month of approval (June 2021) to March 2023. Data on prior ASM usage were collated alongside clinical data, which included seizure frequency and drug load reduction outcomes to March 2025.
Results: Prior to CNB initiation, patients at both office-based practices had similar levels of 1-2 concurrent ASMs (Berlin 80%; Hamburg 77%). The most common ASMs were voltage-gated sodium channel blockers (VGSC), Levetiracetam (LEV)/Brivaracetam (BRV) synaptic vesicle protein 2A (SV2A) inhibitors, and Perampanel (PER). CNB titration was configured into a quarterly office-based outpatient schedule. All patients had seizure reductions in-line with published and real-world evidence, and were compliant.
Discussion and conclusion: CNB is a valuable adjunctive therapy suitable for refractory epilepsy outpatients attending office-based neurologists. A slow titration schedule helped mitigate most side effects. Despite differences to clinic-based practice, in office-based outpatient practice CNB can be broadly used. It can be prescribed to patients on conventional therapy who are still having seizures and have failed two or more other ASMs. By reporting experiences of CNB titration, seizure, and drug load reduction outcomes in office-based neurology, this study will give German office-based outpatient neurologists evidence to support both CNB and other third-generation ASM use in their practice.
Keywords: Cenobamate; antiseizure medication; epilepsy care pathways; epileptologist; neurologist; outpatients; refractory epilepsy; seizure freedom.
Copyright © 2025 House and Wiese.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Pfäfflin M, Stefan H, May TW. Wie viele Patienten mit Epilepsie gibt es in Deutschland, und wer behandelt sie? Z Epileptol. (2020) 33:218–25. doi: 10.1007/s10309-020-00334-8 - DOI
-
- Willems LM, Hamer HM, Knake S, Rosenow F, Reese JP, Strzelczyk A. General trends in prices and prescription patterns of anticonvulsants in Germany between 2000 and 2017: analysis of national and cohort-based data. Appl Health Econ Health Policy. (2019) 17:707–22. doi: 10.1007/s40258-019-00487-2, PMID: - DOI - PubMed
-
- Hochbaum M, Kienitz R, Rosenow F, Schulz J, Habermehl L, Langenbruch L, et al. Trends in antiseizure medication prescription patterns among all adults, women, and older adults with epilepsy: a German longitudinal analysis from 2008 to 2020. Epilepsy Behav. (2022) 130:108666. doi: 10.1016/j.yebeh.2022.108666, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources