

Lymphocyte-to-high-density lipoprotein ratio and mortality in asthma patients: a novel immunoinflammatory biomarker with nonlinear association
- PMID: 40584718
- PMCID: PMC12202334
- DOI: 10.3389/fmed.2025.1553188
Lymphocyte-to-high-density lipoprotein ratio and mortality in asthma patients: a novel immunoinflammatory biomarker with nonlinear association
Abstract
Background: The lymphocyte-to-high-density lipoprotein ratio (LHR), a novel biomarker reflecting systemic inflammation and immune status, has been widely studied in various diseases. However, its association with mortality risk among asthma patients remains unexplored.
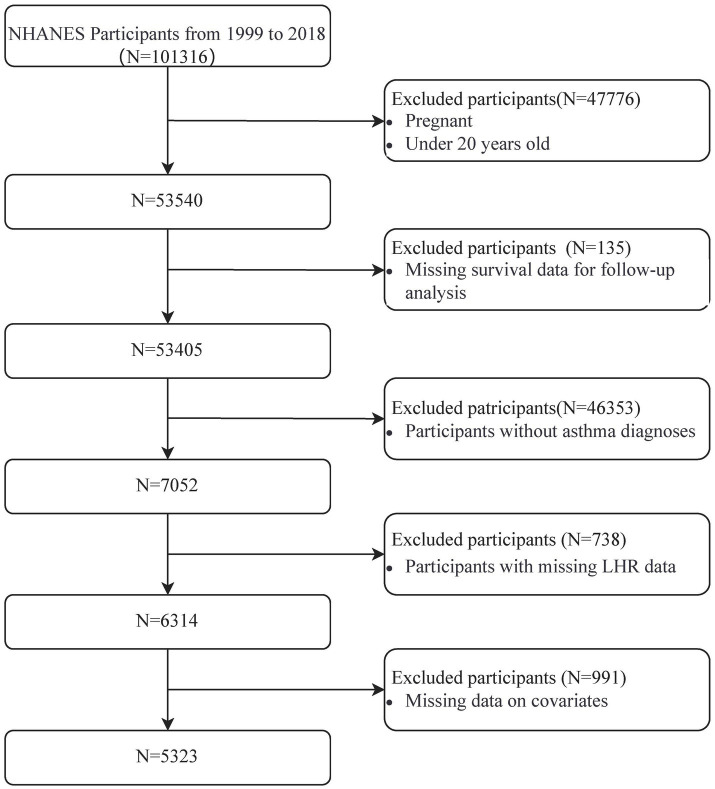
Methods: This study utilized data from the National Health and Nutrition Examination Survey (NHANES) spanning 1999-2018, including 5,323 adult asthma patients. Mortality outcomes were ascertained through linkage with the National Death Index (NDI) up to December 31, 2019. Cox proportional hazards models and Fine-Gray competing risk models were employed to examine the association between LHR and mortality risks. Dose-response relationships were assessed using restricted cubic spline analyses.
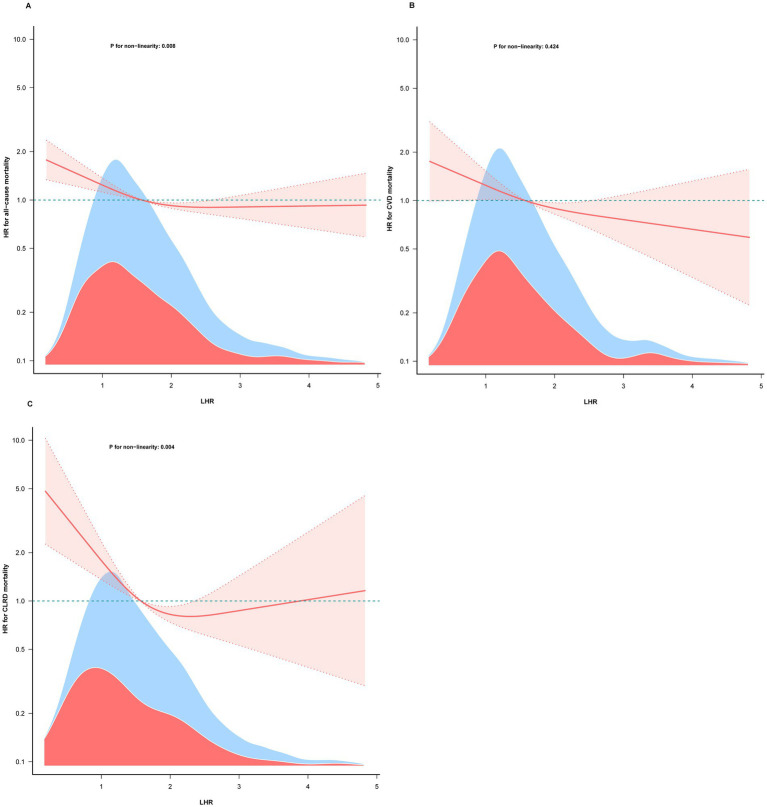
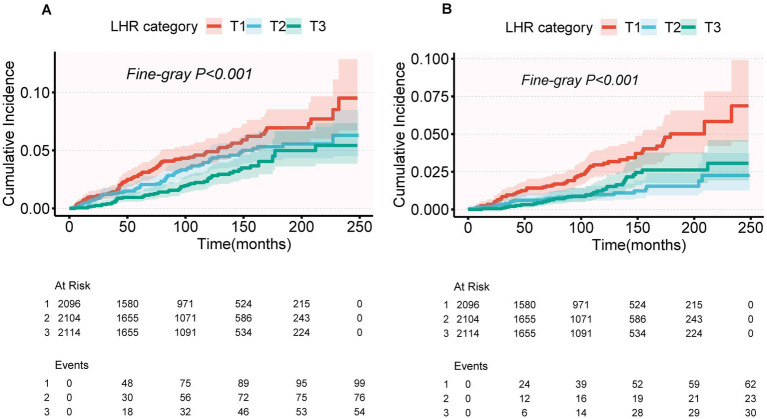
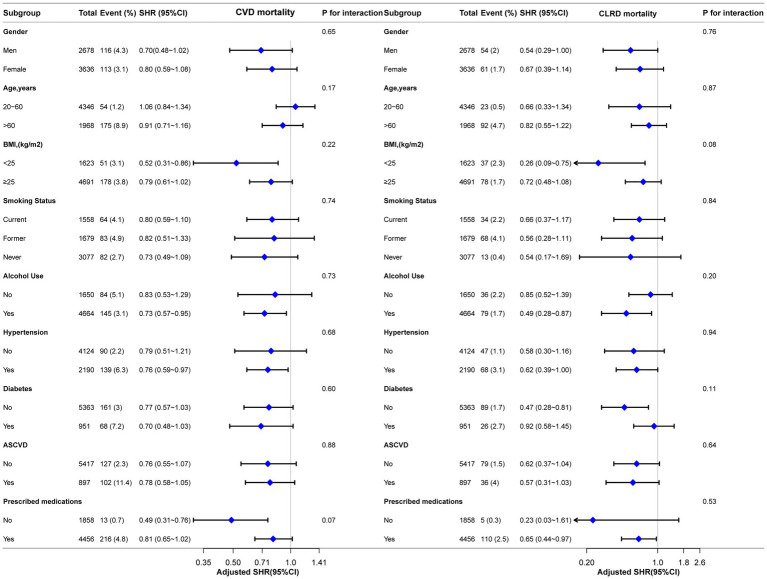
Results: Over a mean follow-up period of 106.95 months, 724 all-cause deaths (13.6%) were recorded. After multivariable adjustment, a one-unit increase in log-transformed LHR was associated with reduced risks of mortality: 18% for all-cause (HR = 0.82, 95% CI: 0.74-0.91), 21% for cardiovascular disease (CVD) (HR = 0.79, 95% CI: 0.65-0.96), and 41% for chronic lower respiratory disease (CLRD) (HR = 0.59, 95% CI: 0.45-0.77). Restricted cubic spline analyses showed an L-shaped association of LHR with all-cause and CLRD mortality, with inflection points at 1.78 and 1.52, respectively. For CVD mortality, a linear association was observed. Competing risk models further confirmed the association of LHR with reduced CLRD mortality (SHR = 0.64, 95% CI: 0.46-0.88), while the association with CVD mortality was no longer significant (SHR = 0.85, 95% CI: 0.70-1.03).
Conclusion: LHR is nonlinearly associated with all-cause and CLRD mortality and shows a significant inverse association with CLRD mortality risk. These findings were further validated using competing risk models, highlighting the robustness of the results.
Keywords: NHANES; asthma; competing risk analysis; lymphocyte-to-high-density lipoprotein ratio (LHR); mortality.
Copyright © 2025 Tian, Wu, Xie, Qu, Wang and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Association between albumin to globulin ratio and all-cause and cardiovascular mortality among individuals with cardiovascular-kidney-metabolic syndrome: results from NHANES 2003 to 2018.Front Nutr. 2025 Jul 3;12:1622590. doi: 10.3389/fnut.2025.1622590. eCollection 2025. Front Nutr. 2025. PMID: 40678773 Free PMC article.
-
Elevated pulse wave velocity as a marker of arterial stiffness and its association with mortality in US adults.Sci Rep. 2025 Jul 2;15(1):23026. doi: 10.1038/s41598-025-07198-w. Sci Rep. 2025. PMID: 40596198 Free PMC article.
-
Association of C reactive protein triglyceride glucose index with mortality in coronary heart disease and type 2 diabetes from NHANES data.Sci Rep. 2025 Jul 9;15(1):24687. doi: 10.1038/s41598-025-10184-x. Sci Rep. 2025. PMID: 40634472 Free PMC article.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
References
-
- Global Initiative for Asthma . Global Strategy for Asthma Management and Prevention, (2024). Available online at: www.ginasthma.org
-
- World Health Organization . Asthma fact sheet, (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/asthma
-
- Al Ghobain MO, Alsubaie AS, Aljumah WA, Alrumayh FM, Aldawsari KF, Alqahtani AM, et al. The correlation between fractional exhaled nitric oxide (FeNO), blood eosinophil count, immunoglobulin E levels, and spirometric values in patients with asthma. Cureus. (2023) 15:e35289. doi: 10.7759/cureus.35289, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous