

Assessing the Causal Effect of Pulse Pressure on Migraine Risk: A Mendelian Randomization Study
- PMID: 40584772
- PMCID: PMC12206417
- DOI: 10.2147/JPR.S512795
Assessing the Causal Effect of Pulse Pressure on Migraine Risk: A Mendelian Randomization Study
Abstract
Background: Migraine is notably prevalent among young individuals and women, who generally demonstrate favorable arterial compliance. Pulse pressure is a reliable measure of arterial compliance; nevertheless, the association between pulse pressure and migraine is not well understood.
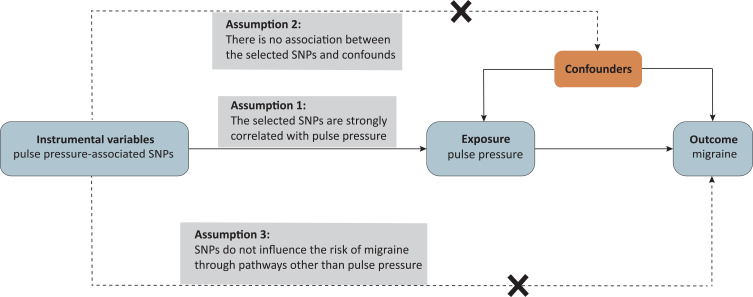
Aim: To investigate the potential causal relationship between pulse pressure and the risk of migraine using Mendelian randomization (MR).
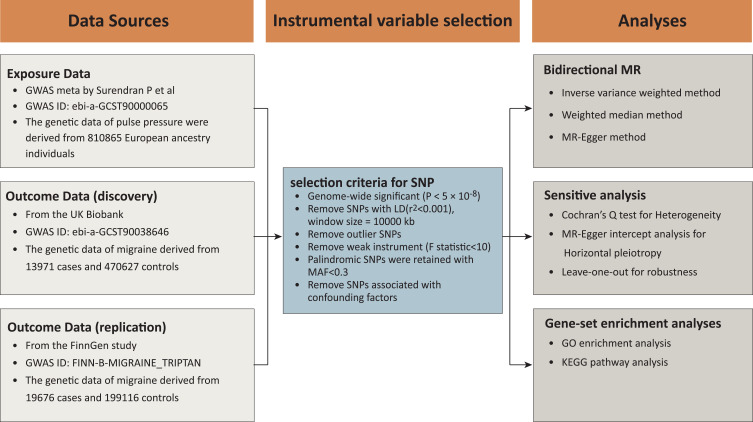
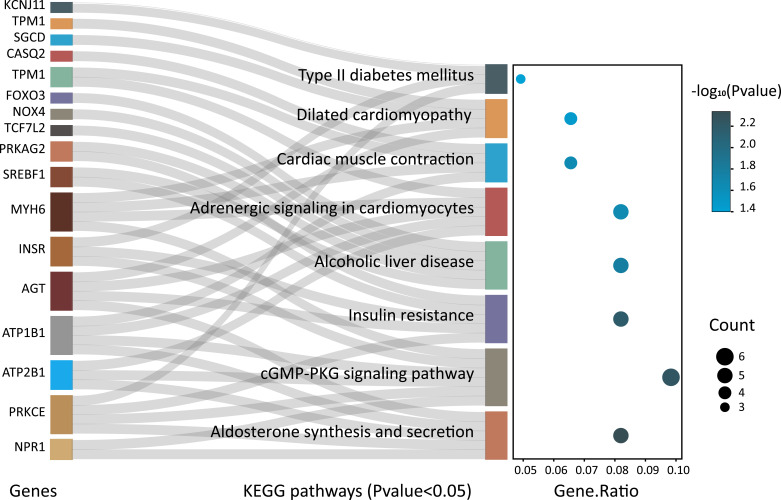
Methods: The pulse pressure studies mainly involved participants of European descent, while the migraine studies included individuals from various parts of the UK. The primary analysis used Inverse Variance Weighted (IVW) method, supplemented by weighted median and MR-Egger regression. Validation data came from the FinnGen study. Genes linked to pulse pressure were analyzed for Gene Ontology (GO) and KEGG enrichment using the DAVID platform.
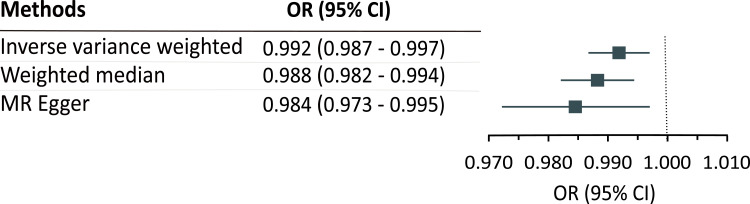
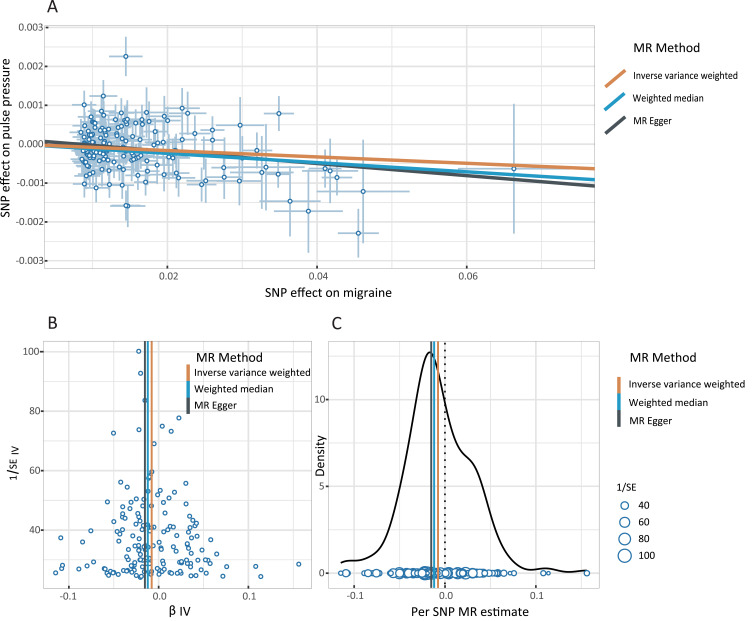
Results: Single-nucleotide polymorphisms linked to pulse pressure were sourced from a GWAS database (810,865 individuals), while migraine data came from UK Biobank (13,971 cases, 470,627 controls). The IVW method showed an OR of 0.992 [95% confidence interval (CI), 0.987-0.997; p = 0.002]. Both weighted median (OR 0.988; 95% CI, 0.982-0.994; p < 0.001) and MR-Egger (OR 0.985; 95% CI, 0.972-0.997; p = 0.016) analyses confirmed a negative causal link between pulse pressure and migraine risk. The MR-Egger intercept analysis showed minimal evidence of horizontal pleiotropy (b = 0.00013, SE = 0.00010, p = 0.209). Finnish data confirmed a causal link between migraine and pulse pressure, with the IVW method indicating a significant association (OR = 0.790, 95% CI: 0.676-0.922; p = 0.003). KEGG enrichment analysis revealed significant pathways regulating pulse pressure, many related to cardiovascular disease and type 2 diabetes.
Conclusion: MR analysis showed that pulse pressure causally affects migraines, potentially explaining why young people and women experience more migraines, while those with type 2 diabetes have a lower risk. Further research is needed to understand this relationship.
Keywords: Mendelian randomization; causal association; gwas; migraine; pulse pressure.
© 2025 Xu et al.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
