

Cardiovascular magnetic resonance imaging and endomyocardial biopsy in giant cell myocarditis: a case report on diagnostic challenges and future perspectives
- PMID: 40585196
- PMCID: PMC12204184
- DOI: 10.1093/ehjcr/ytaf276
Cardiovascular magnetic resonance imaging and endomyocardial biopsy in giant cell myocarditis: a case report on diagnostic challenges and future perspectives
Abstract
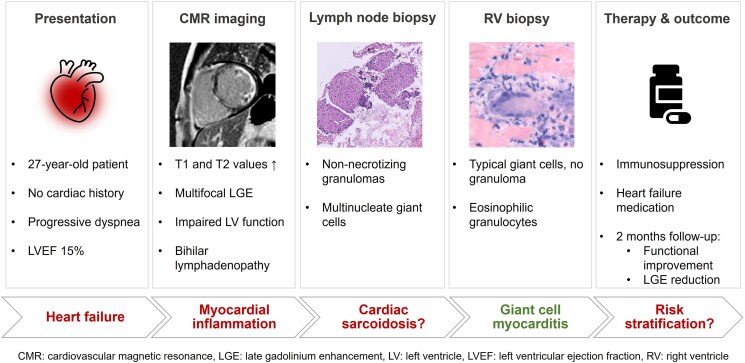
Background: Giant cell myocarditis (GCM) is a rare but often fast-progressing cardiac disease with a high risk of poor outcome. Nonetheless, its differentiation from other diseases like cardiac sarcoidosis (CS) using cardiovascular magnetic resonance imaging (CMR) remains challenging.
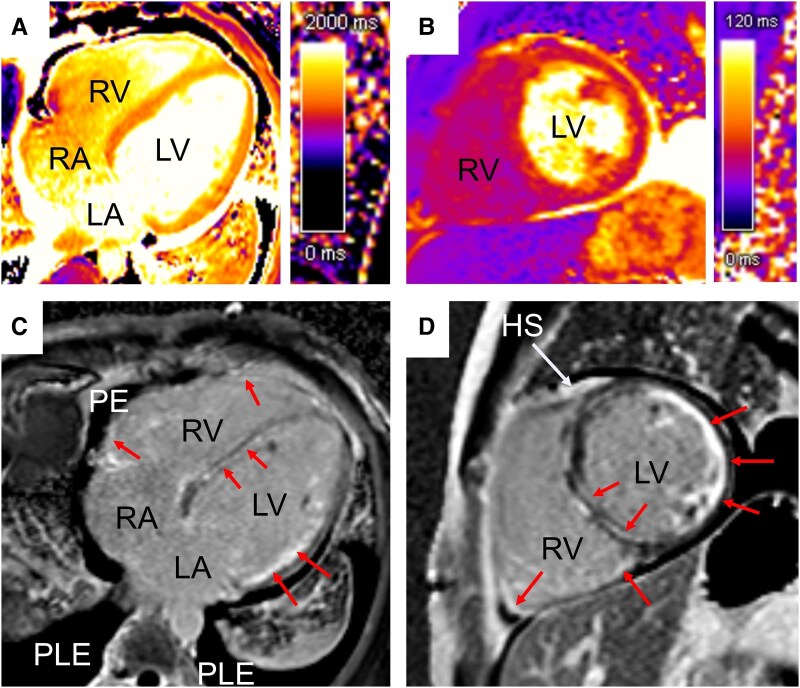
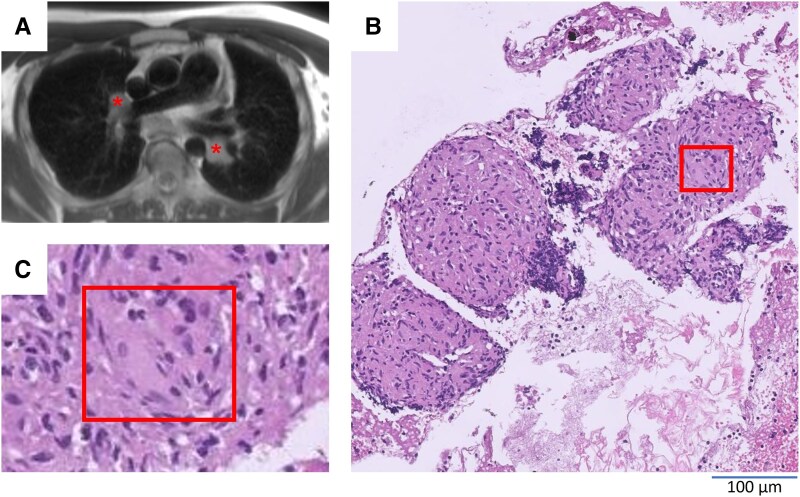
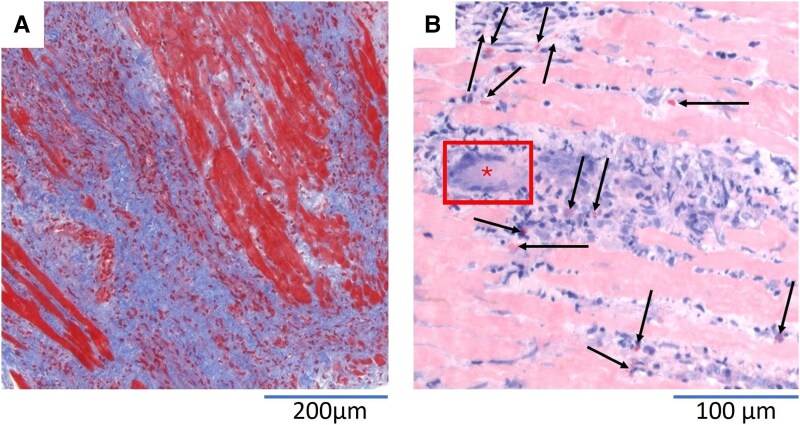
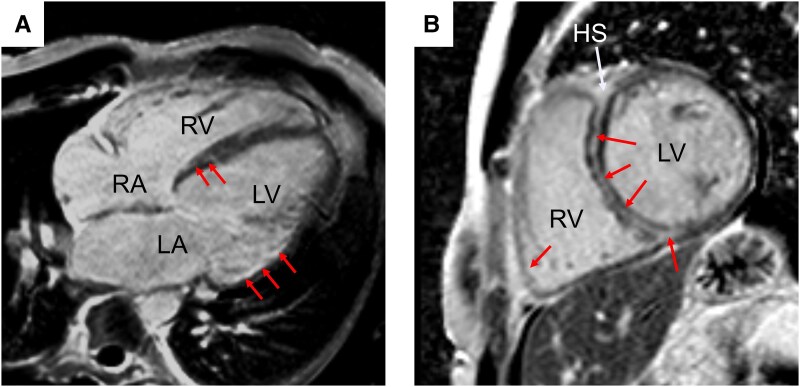
Case summary: A 27-year-old male patient presented to the emergency department with acute cardiac decompensation and severely reduced left ventricular ejection fraction. After exclusion of an ischaemic cause of heart failure, CMR was performed, showing signs of acute inflammation and late gadolinium enhancement patterns that were indistinguishable between GCM and CS. Despite the suspicion of sarcoidosis based on a lymph node biopsy, endomyocardial biopsy (EMB) provided clear evidence of typical histopathological changes consistent with GCM. An immunosuppressive therapy was initiated leading to an improvement in left ventricular function.
Discussion: Cardiovascular magnetic resonance imaging is an important cornerstone in the diagnostic pathway of GCM, however, only complementary use with EMB allows reliable diagnosis. Therefore, full diagnostic and especially prognostic potential of CMR remains unclear but offers an important starting point for optimizing patient management.
Keywords: Cardiovascular magnetic resonance; Case report; Histopathology; Multimodal imaging; Myocarditis; Sarcoidosis.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest. None declared.
Figures
Similar articles
-
Recurrent Cardiac Sarcoidosis and Giant Cell Myocarditis After Heart Transplant: A Case Report and Systematic Literature Review.Am J Cardiol. 2023 Nov 15;207:271-279. doi: 10.1016/j.amjcard.2023.08.005. Epub 2023 Sep 26. Am J Cardiol. 2023. PMID: 37769570
-
Validating real-time three-dimensional echocardiography against cardiac magnetic resonance, for the determination of ventricular mass, volume and ejection fraction: a meta-analysis.Clin Res Cardiol. 2024 Mar;113(3):367-392. doi: 10.1007/s00392-023-02204-5. Epub 2023 Apr 20. Clin Res Cardiol. 2024. PMID: 37079054 Free PMC article.
-
A Case Report: The Utility of Multimodality Imaging in the Diagnosis of Cardiac Sarcoidosis-Has It Surpassed the Need for a Biopsy?Reports (MDPI). 2025 Mar 6;8(1):28. doi: 10.3390/reports8010028. Reports (MDPI). 2025. PMID: 40729241 Free PMC article.
-
The utility of cardiac magnetic resonance imaging in the diagnosis of adult patients with acute myocarditis: a systematic review and meta-analysis.Int J Cardiol. 2022 Sep 15;363:225-239. doi: 10.1016/j.ijcard.2022.06.047. Epub 2022 Jun 18. Int J Cardiol. 2022. PMID: 35724801
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.Health Technol Assess. 2006 Dec;10(49):iii-iv, ix-xi, 1-157. doi: 10.3310/hta10490. Health Technol Assess. 2006. PMID: 17134597
References
-
- Bobbio E, Bollano E, Oldfors A, Hedner H, Björkenstam M, Svedlund S, et al. Phenotyping of giant cell myocarditis versus cardiac sarcoidosis using cardiovascular magnetic resonance. Int J Cardiol 2023;387:131143. - PubMed
-
- Bang V, Ganatra S, Shah SP, Dani SS, Neilan TG, Thavendiranathan P, et al. Management of patients with giant cell myocarditis: JACC review topic of the week. J Am Coll Cardiol 2021;77:1122–1134. - PubMed
Publication types
LinkOut - more resources
Full Text Sources