

Neurocysticercosis in a Non-Endemic Region: A Retrospective Cohort Study at Sheikh Khalifa Medical City (SKMC), Abu Dhabi, UAE
- PMID: 40585698
- PMCID: PMC12206390
- DOI: 10.7759/cureus.85082
Neurocysticercosis in a Non-Endemic Region: A Retrospective Cohort Study at Sheikh Khalifa Medical City (SKMC), Abu Dhabi, UAE
Abstract
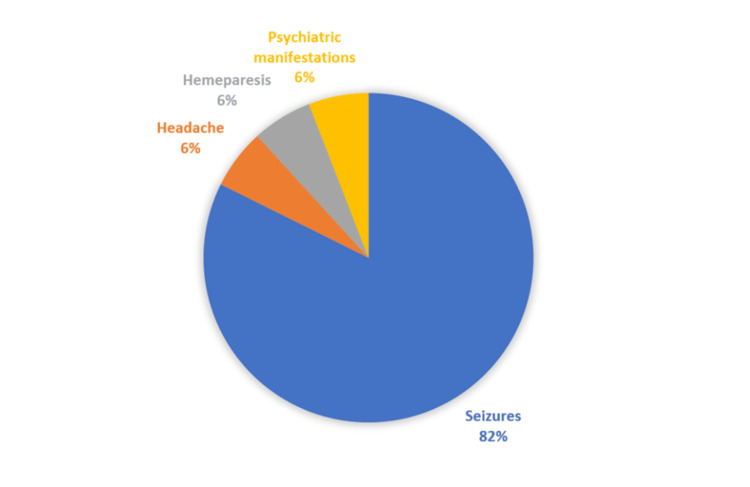
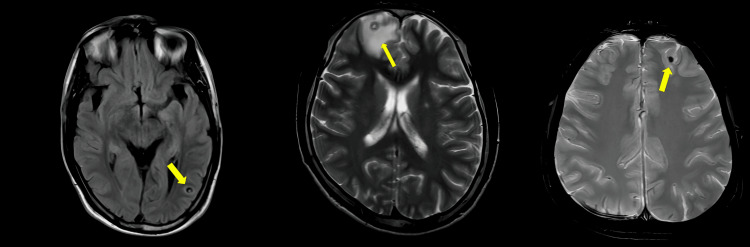
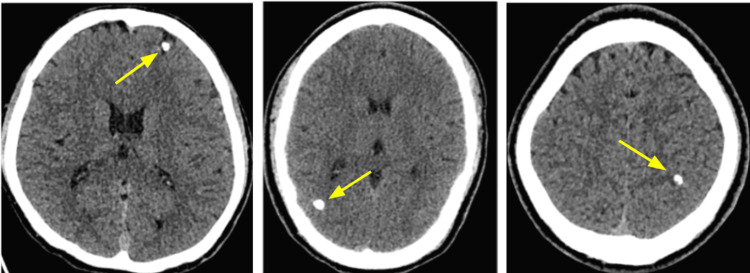
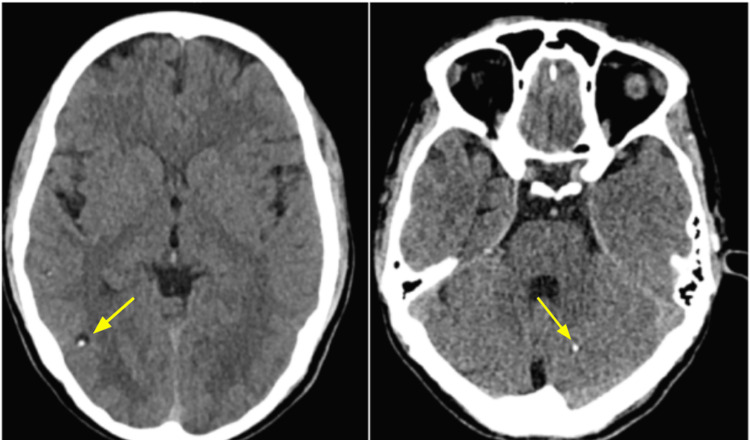
Introduction Neurocysticercosis (NCC) is the most common parasitic disease of the nervous system and a leading cause of acquired epilepsy. To our knowledge, this is the first study to describe the clinical presentation, radiological manifestations, short-term outcomes, and treatment of patients diagnosed with neurocysticercosis (NCC) at a tertiary care center in the United Arab Emirates (UAE), conducted at Sheikh Khalifa Medical City (SKMC), Abu Dhabi. This study aims to describe the demographics, presenting symptoms, neuroimaging patterns, and treatment responses of patients diagnosed with NCC in a non-endemic setting over a 10-year period. This study also aims to improve healthcare provider awareness of neurocysticercosis in a non-endemic region. Methods A retrospective review was conducted using the charts from the electronic medical records of adult patients (>16 years of age) with confirmed diagnosis of NCC who were admitted to SKMC between January 1, 2012 and December 31, 2021. Demographic data, symptoms at presentation, neuroimaging findings and treatment were retrieved from the medical records of these patients. Results During the period between 2012 and 2021, 17 patients who were eventually diagnosed with NCC were admitted to the medical ward through the emergency department at SKMC. Most patients (n=14, 82.4%) were aged between 16 and 37 years. Only one patient was female (n=1, 5.9%), yielding a male-to-female ratio of 16:1. All patients were from Southeast Asia, with the majority (n=12, 70.6%) originating from India. The main presenting symptom was generalized tonic-clonic seizures, observed in 14 (82.4%) patients. These patients were started on antiepileptic drugs (AEDs) after the diagnosis of NCC was confirmed. They were advised to follow up with their primary care physician for ongoing management and continuation of care. Other presenting symptoms were equally seen, including hemiparesis (n=1, 5.9%), headaches (n=1, 5.9%), and psychiatric manifestations (n=1, 5.9%). All patients (100%) had a Computed Tomography (CT) head done on admission, and all of them had cysts typical of NCC on their imaging studies. Eleven patients (n=11, 64.7%) had one cyst only, while three (n=3, 17.6%) had more than four cysts. The most common location was the frontal lobe (n=7, 41.2%), followed by the parietal lobe (n=6, 35.3%). In terms of antiparasitic initiation, only one patient was not put on any antiparasitic therapy since he had a calcified lesion. Nine patients (53%) received prednisolone at 1mg/kg/day, tapered over 10 days. Conclusion NCC is a common cause of seizures and should be considered in the differential diagnosis of patients presenting with seizures, particularly in expatriates from endemic regions. Diagnosis should follow standardized criteria such as Del Brutto's, and albendazole remains first-line therapy unless lesions are calcified. While NCC is not directly contagious, its transmission through ingestion of Taenia solium eggs underscores the importance of hand hygiene practices and preventive health education. This study highlights the need for greater clinical awareness and further research to support public health planning in non-endemic settings.
Keywords: cystic brain lesions; cysticercosis; neglected tropical diseases; neurocysticercosis; non-endemic region; taenia solium; uae.
Copyright © 2025, El-Lahawi et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Review Board at Sheikh Khalifa Medical City issued approval IRB#777. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Antiepileptic drugs for seizure control in people with neurocysticercosis.Cochrane Database Syst Rev. 2021 Nov 1;11(11):CD009027. doi: 10.1002/14651858.CD009027.pub4. Cochrane Database Syst Rev. 2021. PMID: 34723391 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
References
LinkOut - more resources
Full Text Sources