

Efficacy and safety of combining Chinese medicine with Western medicine for gallstone treatment
- PMID: 40587666
- PMCID: PMC12212820
- DOI: 10.1097/MD.0000000000043065
Efficacy and safety of combining Chinese medicine with Western medicine for gallstone treatment
Abstract
Background: Background gallstones are a common and multiple disease, with a high global prevalence, complications such as cholecystitis, pancreatitis, and even increased risk of cancer. Oral Chinese medicine, as the main treatment method of traditional Chinese medicine, is widely used in the treatment of gallstones. This study aimed to evaluate the efficacy and safety of Chinese medicine combined with Western medicine for the treatment of gallstones.
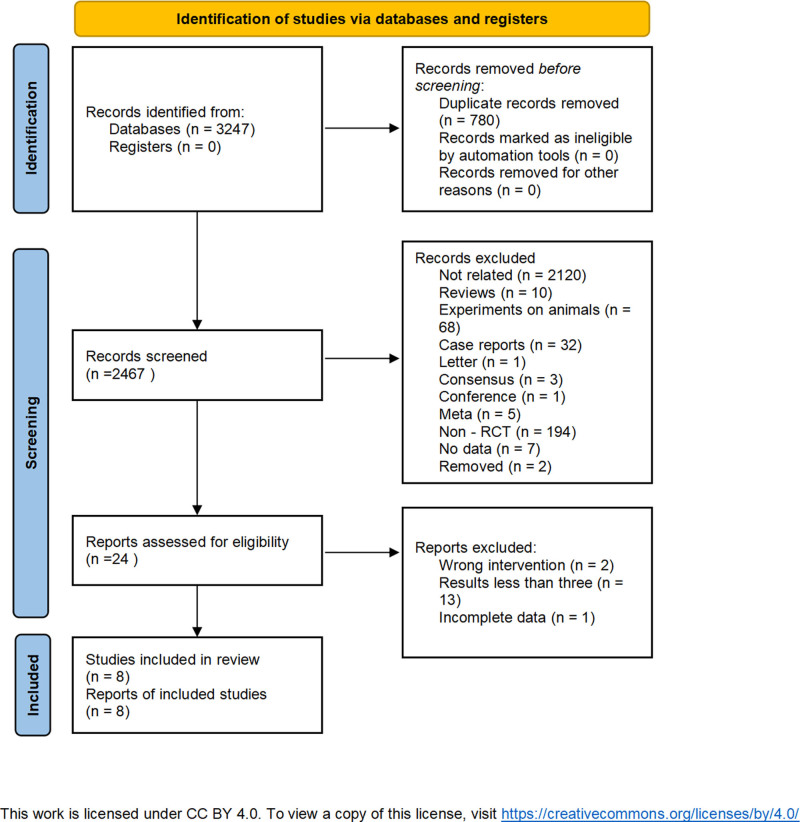
Methods: We searched PubMed, Web of Science, Embase, Cochrane Library, Chinese National Knowledge Infrastructure, WanFang, Chinese Scientific Journal Database (VIP), and Chinese BioMedical Literature Database. The search time was set to be up to July 2, 2024. Data analysis using Revman 5.3 software. The protocol is registered in the PROSPERO database (CRD42024567327).
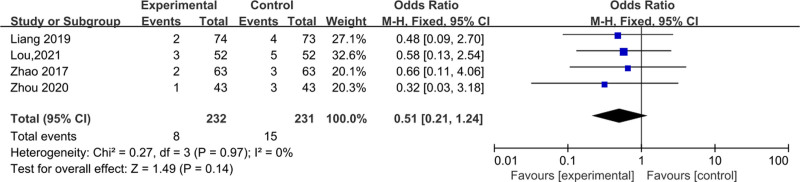
Results: Ultimately, 912 patients from 8 randomized controlled trials were included. The meta-analysis results of traditional Chinese medicine combined with Western medicine versus Western medicine were as follows: imaging examination (standardized mean difference, SMD = -1.51, 95% confidence interval [CI] (-2.36, -0.65), P < .001), total cholesterol level (SMD = -2.14, 95% CI (-3.61, -0.67), P = .004), total bile acid level (SMD = -0.97, 95% CI (-3.36, -1.42), P = .043), traditional Chinese medicine symptom scores (SMD = -1.88, 95% CI (-3.16, -0.60), P = .004), occurrence of adverse reaction (odds ratio = 0.51, 95% CI (0.21, 1.24), P = .14).
Conclusion: The curative effect of Chinese medicine combined with Western medicine in the treatment of gallstones is better than that of Western medicine and is safety. Due to the limited quantity and quality of the included literature, more literature on double-blind randomized controlled trials with large samples is needed in the later stage to verify this conclusion.
Keywords: Western medicine; gallstones; meta-analysis; systematic review; traditional Chinese medicine.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures




References
-
- Wang X, Yu W, Jiang G, et al. Global epidemiology of gallstones in the 21st Century: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2024;22:1586–95. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
