

Severe rhabdomyolysis induced by bezafibrate in the treatment of severe acute pancreatitis with hyperlipidemia: A case report
- PMID: 40587712
- PMCID: PMC12212782
- DOI: 10.1097/MD.0000000000043009
Severe rhabdomyolysis induced by bezafibrate in the treatment of severe acute pancreatitis with hyperlipidemia: A case report
Abstract
Rationale: The important etiological treatment for hyperlipidemic severe acute pancreatitis is to reduce blood lipid. Statins or fibrates are often selected in clinical practice. Most reports indicate that statins or statin combination therapy can cause serious complications such as rhabdomyolysis syndrome (RM) and even poor prognosis. However, in fact, RM may also occur when fibrates alone are used to reduce blood lipid.
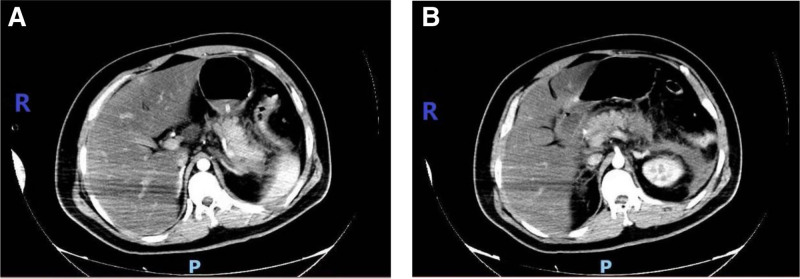
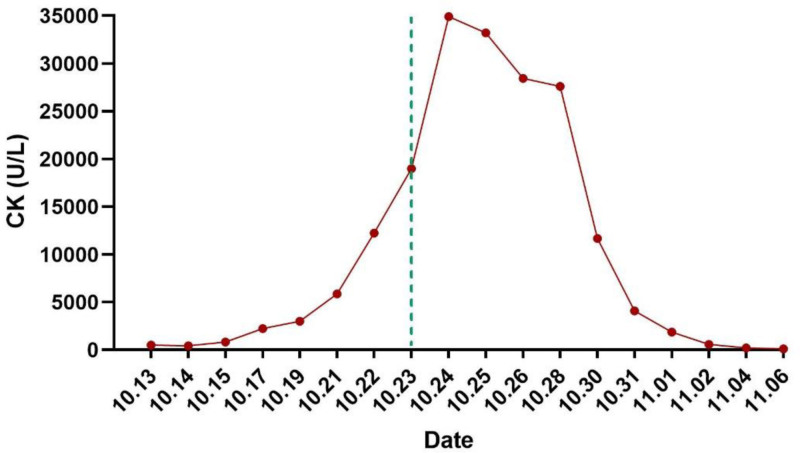
Patient concerns: A 25-year-old man was admitted to our hospital for a 2-day history of abdominal pain, nausea, and vomiting. This patient presented with typical clinical manifestations of acute pancreatitis such as abdominal pain, abdominal distension, nausea, vomiting, and difficulty in defecation after a greasy diet. Auxiliary examinations such as blood (urine) amylase, lipase, blood lipid, abdominal computed tomography, and color Doppler ultrasound confirmed hyperlipidemic severe acute pancreatitis. However, after admission, during the treatment for reducing blood lipid, the blood creatine kinase index of the patient continued to increase, reaching more than 200 times the upper limit of normal at the highest. Accompanied by typical clinical manifestations, rhabdomyolysis was considered. After discussions among experts in the department, differentiations were mainly made from drugs after admission, recent history of toxicant exposure, history of trauma, past history of similar rhabdomyolysis, and other etiologies causing elevated myocardial enzyme spectrum. Finally, it was considered related to bezafibrate.
Diagnoses: RM.
Interventions: Bezafibrate tablets for lowering blood lipids were immediately discontinued. On the second day after discontinuation, there was a small decrease in creatine kinase. Then, appropriate fluid infusion, alkalinization of urine, addition of plasma exchange, and bedside continuous renal replacement therapy were administered.
Outcomes: The level of muscle enzymes decreased progressively and finally returned to normal before discharge.
Lessons: In clinical practice, it is necessary to dynamically monitor the changes of liver and kidney functions and myocardial enzyme spectrum when using bezafibrate tablets to treat hyperlipidemic pancreatitis.
Keywords: bezafibrate; case report; hyperlipidemia; rhabdomyolysis syndrome; severe acute pancreatitis.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Serum amylase and lipase and urinary trypsinogen and amylase for diagnosis of acute pancreatitis.Cochrane Database Syst Rev. 2017 Apr 21;4(4):CD012010. doi: 10.1002/14651858.CD012010.pub2. Cochrane Database Syst Rev. 2017. PMID: 28431198 Free PMC article.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.Health Technol Assess. 2007 Apr;11(14):1-160, iii-iv. doi: 10.3310/hta11140. Health Technol Assess. 2007. PMID: 17408535
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361:62–72. - PubMed
-
- Cabral BMI, Edding SN, Portocarrero JP, Lerma EV. Rhabdomyolysis. Dis Mon. 2020;66:101015. - PubMed
-
- Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet. 2015;386:85–96. - PubMed
-
- Stanley M, Chippa V, Aeddula NR, et al. Rhabdomyolysis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. Bookshelf ID: NBK448168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
