

Circulating Proteins for Prediction of Kidney Disease Progression and Cardiovascular Outcomes: Individual Participant Data Meta-Analysis of Four Cohorts
- PMID: 40587944
- PMCID: PMC12329602
- DOI: 10.1159/000547138
Circulating Proteins for Prediction of Kidney Disease Progression and Cardiovascular Outcomes: Individual Participant Data Meta-Analysis of Four Cohorts
Abstract
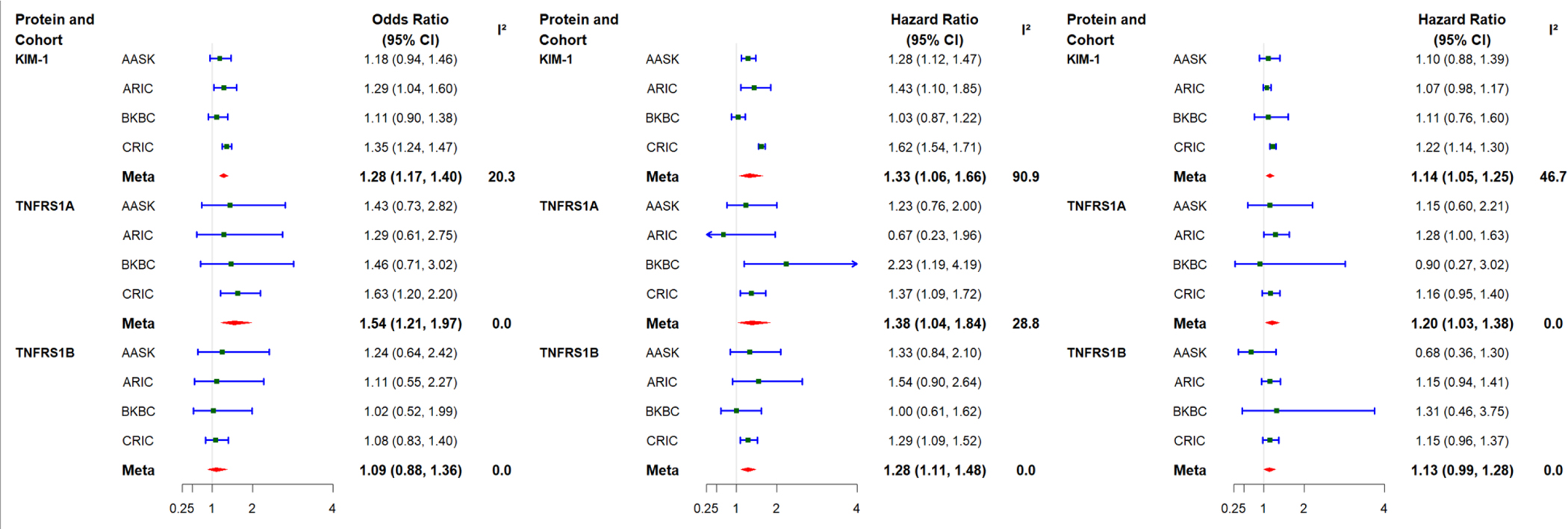
Introduction: KIM-1, TNFRSF1A, and TNFRSF1B have been accepted as early risk markers in diabetic kidney disease by the US Food and Drug Administration. Whether they may be useful in identifying high-risk patients for cardiovascular/kidney clinical trial enrollment in other important subgroups is uncertain.
Methods: We evaluated the potential prognostic enrichment of KIM-1, TNFRSF1A, and TNFRSF1B in four cohorts: the Atherosclerosis Risk in Communities (ARIC) (N = 4,594, mean age 76 years, 55% women, mean eGFR 68 mL/min/1.73 m2), African American Study of Kidney Disease and Hypertension (AASK) (N = 705, mean age 55 years, 39% women, mean mGFR 46 mL/min/1.73 m2), Chronic Renal Insufficiency Cohort (CRIC) (N = 2,943, mean age 59 years, 45% women, mean eGFR 35 mL/min/1.73 m2), and Boston Kidney Biopsy Cohort (BKBC) (N = 434, mean age 54 years, 48% women, mean eGFR 51 mL/min/1.73 m2). We evaluated three outcomes: 40% glomerular filtration rate (GFR) decline, kidney failure, and incident cardiovascular disease (CVD) overall and in two subgroups historically underrepresented in clinical trials: participants with no diabetes, and those with albuminuria <200 mg/g.
Results: Published models (40% decline tool, kidney failure risk equation, and PREVENT) using clinical variables had moderate to strong risk discrimination in each cohort: 40% GFR decline, AUROC range: 0.78-0.90; kidney failure, C-statistic range: 0.75-0.93; and CVD, C-statistic range: 0.59-0.79. After addition of biomarkers, there was a small but significant improvement in the meta-analyzed overall population: change in AUROC in 40% GFR decline: 0.02, p < 0.001; change in C-statistic for kidney failure: 0.01, p = 0.02; change in C-statistic for CVD: 0.01, p = 0.03. Among participants without diabetes, the change was statistically significant only for 40% decline; among patient with albuminuria <200 mg/g, the change was statistically significant only for the two kidney outcomes.
Conclusion: KIM-1, TNFRSF1A, and TNFRSF1B may not be strong prognostic enrichment biomarkers over and above clinical risk estimates. Clinical trials should test whether they help with predictive enrichment.
Keywords: KIM-1; Outcomes; TNFRSF1A; TNFRSF1B.
© 2025 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Conflict of Interest Statement:
Dr. Bonventre is a co-inventor on KIM-1 patents assigned to Mass General Brigham. He is a consultant to Sarepta, Praxis, Nimbus and GentiBio and owns equity in Innoviva, MediBeacon, DxNow, Verinano, Autonomous Medical Devices and Renalytix. The data supporting the findings of this study are openly available through the NIDDK Biorepository. Summary statistics are fully presented in the supplement, and the code to generate these statistics is available on request. Matthew R. Weir was a member of the journal’s Editorial Board at the time of submission.
Figures
References
-
- Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet Lond Engl. 2010. Jun 12;375(9731):2073–81. - PMC - PubMed
-
- Ichimura T, Bonventre JV, Bailly V, Wei H, Hession CA, Cate RL, et al. Kidney Injury Molecule-1 (KIM-1), a Putative Epithelial Cell Adhesion Molecule Containing a Novel Immunoglobulin Domain, Is Up-regulated in Renal Cells after Injury*. J Biol Chem. 1998. Feb 13;273(7):4135–42. - PubMed
Grants and funding
- U01 DK060963/DK/NIDDK NIH HHS/United States
- U01 DK103225/DK/NIDDK NIH HHS/United States
- R01 DK119199/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- 75N92022D00001/HL/NHLBI NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- 75N92022D00002/HL/NHLBI NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R37 DK039773/DK/NIDDK NIH HHS/United States
- 75N92022D00004/HL/NHLBI NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- K24 HL155861/HL/NHLBI NIH HHS/United States
- R01 DK072381/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- 75N92022D00003/HL/NHLBI NIH HHS/United States
- R01 DK108803/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- R01 DK124399/DK/NIDDK NIH HHS/United States
- 75N92022D00005/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
