

Respiratory Burden in Hematology-Related Bronchiectasis: Clinical Characteristics and Treatable Traits
- PMID: 40587956
- PMCID: PMC12313156
- DOI: 10.1159/000547175
Respiratory Burden in Hematology-Related Bronchiectasis: Clinical Characteristics and Treatable Traits
Abstract
Introduction: Hematological conditions, mainly allogeneic hematopoietic cell transplantation (allo-HCT) and chronic lymphocytic leukemia (CLL), have known associations with bronchiectasis. However, data on these unique clinical entities remain limited. We aimed to evaluate the clinical characteristics and outcomes of patients with hematology-related bronchiectasis.
Methods: This retrospective study included patients with bronchiectasis following allo-HCT and CLL. Groups were matched and compared to a control group of bronchiectasis from non-hematological conditions (n = 126). Clinical variables, radiologic features, and disease outcomes were analyzed.
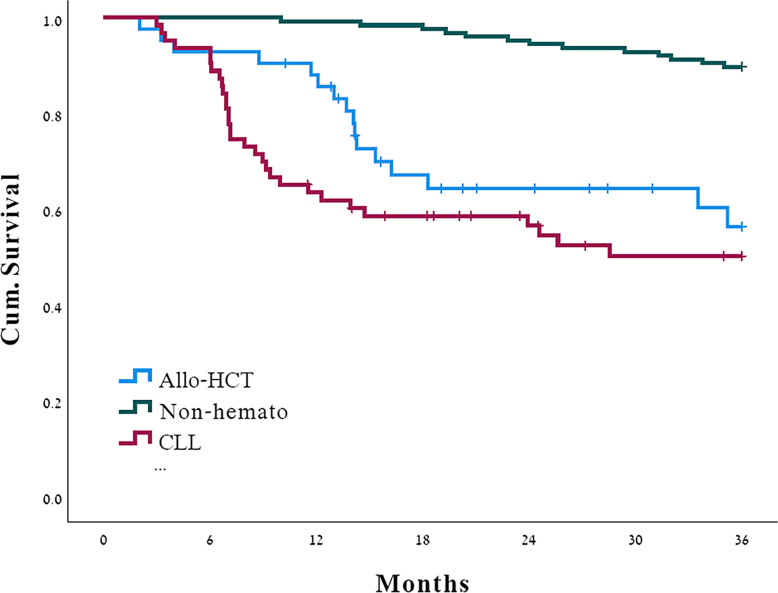
Results: Overall, 42 patients with bronchiectasis after allo-HCT (median age 59, 36% female) and 63 patients with bronchiectasis and CLL (median age 72, 40% female) were included. Both groups exhibited worse lung functions compared to the control. They had more isolations of Pseudomonas aeruginosa (PA) compared to the control group (21-31% vs. 9%) and less non-tuberculosis mycobacteria (3-5% vs. 21%). Allo-HCT and CLL patients also showed high rates of diffuse bronchiectasis distribution (38% and 40%), hypogammaglobulinemia (41% and 71%), and 1-year respiratory hospitalizations (50% and 54%). Only 26% of allo-HCT and 35% of CLL patients saw a pulmonologist, and only 14% performed routine airway clearance. Mortality was higher in both groups compared to controls. The key variables associated with mortality were bronchiolitis obliterans syndrome in the allo-HCT group (HR 11.1, 95% CI: 2.9-30.6) and PA isolation in the CLL group (HR 2.96, 95% CI: 1.3-6.8).
Conclusion: Hematology-related BE have distinct clinical and radiologic features with associated morbidity. These findings could help identify at-risk subgroups for early pulmonologist referral.
Keywords: Bone marrow transplantation; Bronchiectasis; Immunoglobulin; Leukemia; Pseudomonas; Pulmonologists.
© 2025 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
A.B.-S. reports receiving consulting and lecture fees from Boehringer Ingelheim Ltd., GSK, AstraZeneca, Sanofi- Regeneron, Kamada Ltd., and Roche. All other authors report no conflict of interests.
Figures

References
-
- Hill AT, Sullivan AL, Chalmers JD, De Soyza A, Elborn SJ, Floto AR, et al. British thoracic society guideline for bronchiectasis in adults. Thorax. 2019;74(Suppl 1):1–69. - PubMed
-
- King P. Pathogenesis of bronchiectasis. Paediatr Respir Rev. 2011;12(2):104–10. - PubMed
-
- Chalmers JD, Polverino E, Crichton ML, Ringshausen FC, De Soyza A, Vendrell M, et al. Bronchiectasis in Europe: data on disease characteristics from the European Bronchiectasis registry (EMBARC). Lancet Respir Med. 2023;11(7):637–49. - PubMed
-
- Araújo D, Shteinberg M, Aliberti S, Goeminne PC, Hill AT, Fardon T, et al. Standardised classification of the aetiology of bronchiectasis using an objective algorithm. Eur Respir J. 2017;50(6):1701289. - PubMed
LinkOut - more resources
Full Text Sources
