

Efficacy of pembrolizumab and vorinostat combination in patients with recurrent and/or metastatic squamous cell carcinomas: a phase 2 basket trial
- PMID: 40588522
- PMCID: PMC12380617
- DOI: 10.1038/s43018-025-01004-2
Efficacy of pembrolizumab and vorinostat combination in patients with recurrent and/or metastatic squamous cell carcinomas: a phase 2 basket trial
Abstract
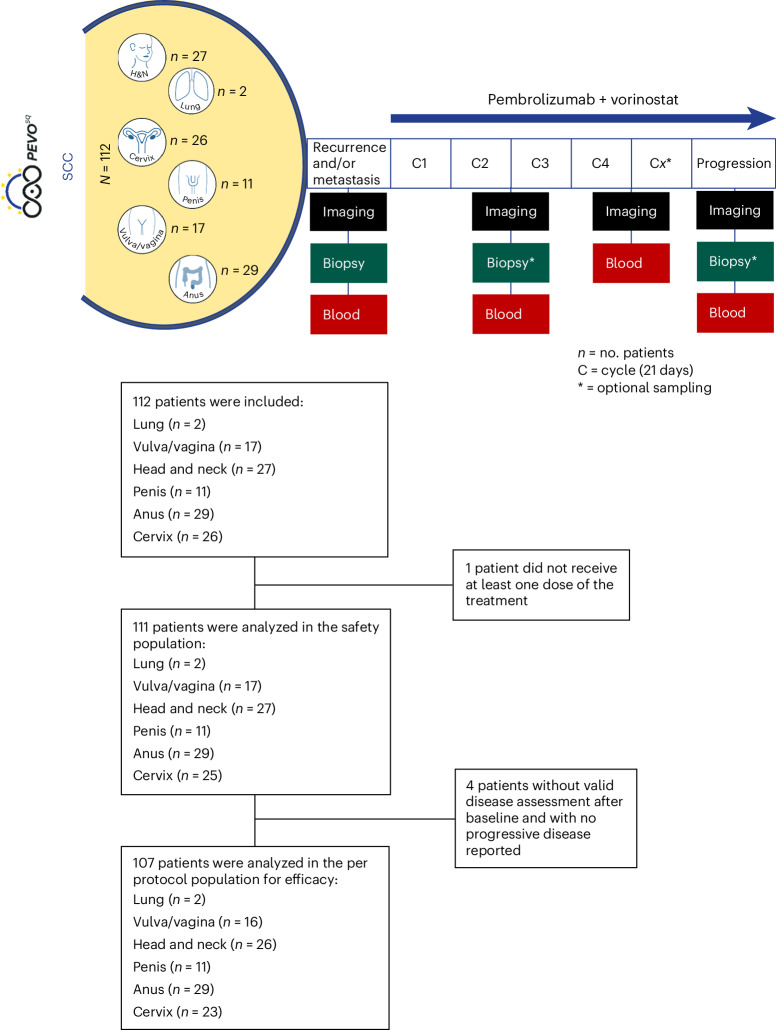
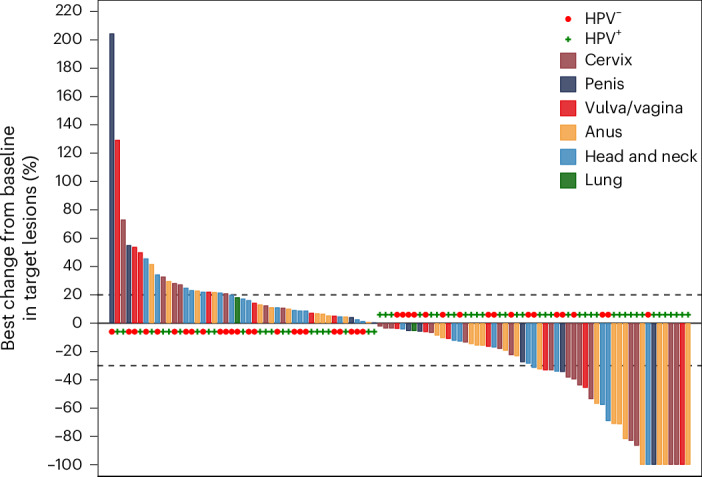
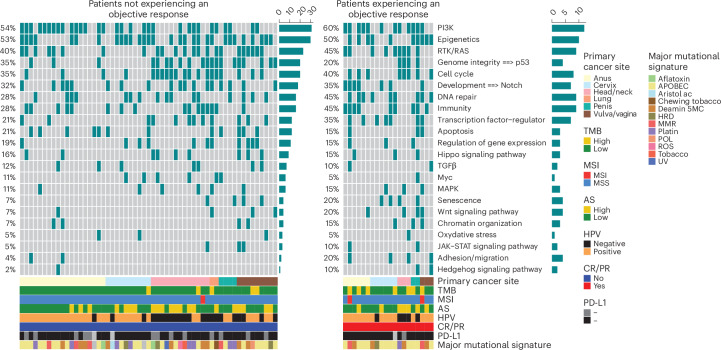
Immune checkpoint inhibitors improve the treatment of many solid tumors and have shown encouraging results in advanced squamous cell carcinoma (SCC), yet only a minority of patients respond to immune checkpoint inhibitor monotherapy. We conducted the PEVOsq trial, an open-label, nonrandomized, multicenter, basket phase 2 trial to evaluate the combination of pembrolizumab and vorinostat in recurrent/metastatic SCC of various origins. The primary endpoint was the objective response rate (ORR) in each tumor cohort during treatment as per the investigators' assessment. Secondary endpoints included safety and antitumor activity evaluation in terms of centrally confirmed ORR, progression-free survival, overall survival and duration of response. In the efficacy population (n = 107), the ORR was met in cervical (39%), anal (31%) and vulvar/vaginal (19%) cancer cohorts, but not in head and neck SCC (19%) or penile (18%) cancer cohorts (overall ORR = 26%). Median progression-free survival was 4.0 months (95% confidence interval: 2.6-4.3), and median overall survival was 11.1 months (95% confidence interval: 9.2-17.4). In the safety population, 101 (91%) of 111 patients developed at least one treatment-related adverse event, with 39% and 5.4% of patients experiencing at least one grade 3 and grade 4 treatment-related adverse event, respectively. Vorinostat-related toxicity prompted a dose reduction/interruption in 66% of patients. Whole-exome sequencing analyses revealed several potential predictive biomarkers of response to treatment. Further studies in a larger number of patients are required to validate these findings. ClinicalTrials.gov identifier: NCT04357873 .
© 2025. The Author(s).
Conflict of interest statement
Competing interests: E.B. received honoraria from Eisai, Merck Sharp and Dohme (MSD), Sandoz and Amgen and meetings/travel grants and nonfinancial support from Daiichi Sankyo, Eisai, Amgen, Sandoz, MSD, Bristol Myers Squibb (BMS), Novartis, Pfizer and Roche and has consulted for Egle Tx, all outside of the submitted work. F.G. received fees for oral communication from Eli Lilly, Sanofi, BMS, AstraZeneca and Amgen, received funding for clinical trials from AstraZeneca, received travel grants from Roche France, Amgen and Servier and is an advisory board member for Merck Serono, Amgen, Roche France and Sanofi, all outside of the submitted work. O.L.S. reports honoraria from MSD and Clovis and travel/accommodation/expenses from Eisai. C.C. participated on advisory boards from Amgen, BMS, Merck Serono, Pierre Fabre and Servier and received personal fees from BMS, Merck Serono, Pierre Fabre and Servier and institutional fees from Amgen, AstraZeneca, BMS, Daiichi Sankyo, MSD and ImCore Roche Genentech. C.B. participated on advisory boards from AstraZeneca, Merck Serono and MSD and received personal fees from AstraZeneca, BMS, Merck Serono and MSD. E.S.-B. participated on advisory boards and received travel expenses from MSD and Merck Serono. C.G.-R. has previously received payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing or educational events from BMS, F. Hoffmann-La Roche, Genentech, Foundation Medicine and Pierre Fabre, has supported or attended meetings and/or travel for MSD and F. Hoffmann-La Roche and has participated on a data safety monitoring board or advisory board for Macomics and Pharmamar. E.G.-R. has relevant relationships (advisory fees, honoraria, travel accommodation and expenses, grants and/or nonfinancial support) with AstraZeneca, Exact Sciences, GSK, Illumina, MSD, Novartis, Roche, Sophia Genetics and Thermo Fisher Scientific, unrelated to the current work. T.F. reports receiving personal fees from Jansen outside the submitted work and institutional fees from Roche and Lilly outside the submitted work. C.L.T. participated on advisory boards from MSD, BMS, Merck, AstraZeneca, Celgene, Seattle Genetics, Roche, Novartis, Rakuten, Nanobiotix and GSK. The other authors declare no competing interests.
Figures






References
-
- de Sanjose, S. et al. Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study. Lancet Oncol.11, 1048–1056 (2010). - PubMed
-
- Vermorken, J. B. et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med.359, 1116–1127 (2008). - PubMed
-
- Pujade-Lauraine, E. et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: the AURELIA open-label randomized phase III trial. J. Clin. Oncol.32, 1302–1308 (2014). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- ANR-18-PERM-0010/Agence Nationale de la Recherche (French National Research Agency)
- PGA1RC20190208493/Fondation ARC pour la Recherche sur le Cancer (ARC Foundation for Cancer Research)
- INTER/ERAPerMed/18/13061865/Fonds National de la Recherche Luxembourg (National Research Fund)
- ERAPerMed 2018_PEVODATA_MAZZARELLA/Ministero della Salute (Ministry of Health, Italy)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
